Flush Rate Oxygen as a Makeshift HFNC

Explore This Issue
ACEP Now: December 2025 (Digital)FIGURE 3. Oxygen regulator in our trauma room. Note that the markings on the side stop at 15 liters per minute, but the sticker to the right of the regulator knob indicates a maximum flush rate of 60 to 80 liters per minute. Photo courtesy of Dr. Paul Jansson. (Click to enlarge.)
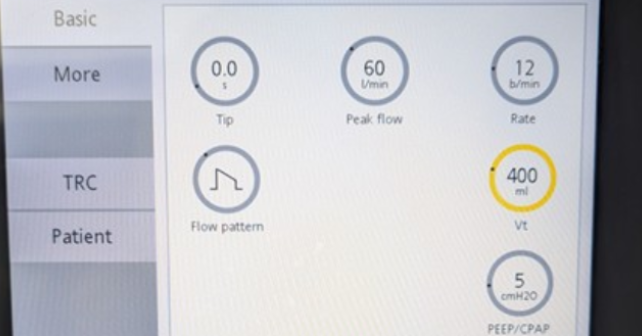
HFNC requires a dedicated device and typically requires a respiratory therapist for initiation, limiting its use for emergent hypoxemia or in out-of-hospital settings.13 If you are waiting for the RT to bring the HFNC, or if you don’t have HFNC at your institution, utilizing flush rate oxygen can approximate the therapy in a pinch. Most wall-mounted regulators have clearly demarcated lines showing the precise amount of oxygen delivered between 0 and 15 liters per minute but are well capable of delivering oxygen past this amount (Figure 3), often up to 60 of 80 liters per minute. At flow rates above 15 LPM, you will not be able to precisely control the flow (nor the FiO2), but you can deliver more oxygen than typically delivered with conventional therapy and more closely match the minute ventilation of the patient. This can be used as a bridge to intubation or noninvasive ventilation,14,15 but should not be utilized for long-term use as the equipment is not designed for the high flow of gas that you are putting through it. The lack of warming and humidification can also be irritating to the upper airway mucosa. Be sure to firmly attach the cannula or NRB mask to the regulator, otherwise it will pop off and make a ferocious noise that will terrify everyone in the room.
 Paul S. Jansson, MD, MS, is the medical director of the emergency critical care center (EC3), director of operations for the division of critical care, and an assistant professor of emergency medicine and internal medicine at the University of Michigan.
Paul S. Jansson, MD, MS, is the medical director of the emergency critical care center (EC3), director of operations for the division of critical care, and an assistant professor of emergency medicine and internal medicine at the University of Michigan.
References
- Levitan RM. Avoid Airway Catastrophes on the Extremes of Minute Ventilation. ACEP Now. Published January 20, 2015. Accessed August 6, 2025. https://www.acepnow.com/article/avoid-airway-catastrophes-extremes-minute-ventilation/.
- Blackie SP, Fairbarn MS, McElvaney NG, Wilcox PG, Morrison NJ, Pardy RL. Normal values and ranges for ventilation and breathing pattern at maximal exercise. Chest. 1991;100(1):136–142.
- Warner MA, Patel B. Mechanical Ventilation. In Benumof and Hagberg’s Airway Management. Third Edition. Elsevier; 2013 981-997.e3.
- Herren T, Achermann E, Hegi T, Reber A, Stäubli M. Carbon dioxide narcosis due to inappropriate oxygen delivery: A case report. J Med Case Rep. Published July 28, 2017. Accessed August 6, 2025.https://jmedicalcasereports.biomedcentral.com/articles/10.1186/s13256-017-1363-7.
- Seeger K. The complete guide to high flow nasal cannula therapy (HFNC). Hamilton Medical. Published December 6, 2024. Accessed August 6, 2025. https://www.hamilton-medical.com/en_US/Article-page~knowledge-base~efb4fa6e-cb67-4e7c-ac50-28b9e3472a04~The-complete-guide-to-high-flow-nasal-cannula-therapy–HFNC-~.html.
- Drake MG. High-flow nasal cannula oxygen in adults: An evidence-based assessment. Ann Am Thorac Soc. Published February 2018. Accessed August 7, 2025. 10.1513/AnnalsATS.201707-548FR.
- Parke RL, Eccleston ML, McGuinness SP. The effects of flow on airway pressure during nasal high-flow oxygen therapy. Respir Care.2011; 56(8):1151–1155.
- Ni YN, Luo J, Yu H, et al. Can High-flow Nasal Cannula Reduce the Rate of Endotracheal Intubation in Adult Patients With Acute Respiratory Failure Compared With Conventional Oxygen Therapy and Noninvasive Positive Pressure Ventilation?: A Systematic Review and Meta-analysis. Chest. 2017;151(4):764–775.
- Frat J-P, Thille AW, Mercat A, et al. High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure. N Engl J Med.2015; [372(23):2185–2196.
- Besnier E, Guernon K, Bubenheim M, et al. Pre-oxygenation with high-flow nasal cannula oxygen therapy and non-invasive ventilation for intubation in the intensive care unit. Intensive Care Med.2016; [42(8):1291–1292.
- Jaber S, Monnin M, Girard M, et al. Apnoeic oxygenation via high-flow nasal cannula oxygen combined with non-invasive ventilation preoxygenation for intubation in hypoxaemic patients in the intensive care unit: the single-centre, blinded, randomised controlled OPTINIV trial. Intensive Care Med. 2016; 42(12):1877–1887.
- Miguel-Montanes R, Hajage D, Messika J, et al. Use of high-flow nasal cannula oxygen therapy to prevent desaturation during tracheal intubation of intensive care patients with mild-to-moderate hypoxemia. Crit Care Med. 2015;43(3):574–583.
- Robinson AE, Pearson AM, Bunting AJ, et al. A Practical Solution for Preoxygenation in the Prehospital Setting: A Nonrebreather Mask with Flush Rate Oxygen. Prehosp Emerg Care. 2024;28(2):215–220.
- Driver BE, Prekker ME, Kornas RL, Cales EK, Reardon RF. Flush Rate Oxygen for Emergency Airway Preoxygenation. Ann Emerg Med. 2017;69(1):1–6.
- Bunting AJ, Driver BE, Pearson AM, et al. Time to adequate preoxygenation when using flush rate oxygen. AmJ Emerg Med.2025;95:63–66.
Pages: 1 2 3 4 | Single Page




No Responses to “Why the Nonrebreather Should be Abandoned”