Enter the Hero…High Flow Nasal Cannula
The high flow nasal cannula (HFNC), also known as the heated, humidified high flow nasal cannula —among other names5 — has revolutionized the treatment of hypoxemic respiratory failure the same way that noninvasive ventilation (NIV) revolutionized the treatment of hypercapnic respiratory failure. The HFNC is a dedicated device that allows for gas flow of up to 60 to 70 liters per minute, compared with up to 6 liters per minute compared to a traditional nasal cannula. With HFNC, you can also precisely adjust the oxygen concentration from 21 percent to 100 percent.
Explore This Issue
ACEP Now: December 2025 (Digital)In addition, these devices also typically heat the air to body temperature and provide humidification, making the high rate of gas flow less irritating to the nasal mucosa and allowing for long-term use. When compared to NRB masks, HFNC is more comfortable, allows the patient to speak and eat, and is a lower aspiration risk.
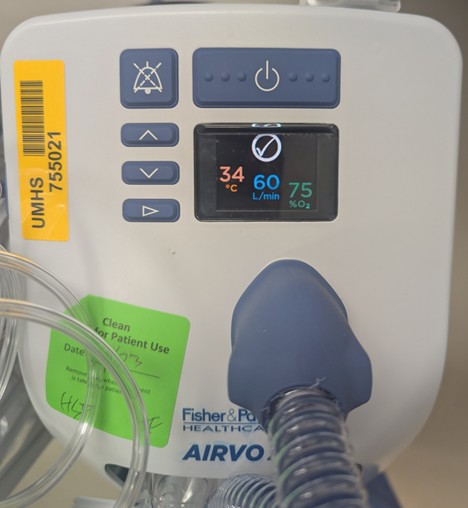
FIGURE 2. High Flow Nasal Cannula controls. Note the temperature (34o C), the flow rate (60 liters per minute), and the FiO2 (75 percent). Photo courtesy of Dr. Paul Jansson. (Click to enlarge.)
In comparison to conventional oxygen delivery devices, HFNC allows for more precise titration of both flow (liters per minute) and oxygenation (FiO2). (Figure 2) When adjusting HFNC, typically the flow is titrated to match the patient’s work of breathing and respiratory rate, while the FiO2 is titrated to match the patient’s oxygen saturation (SpO2).
With much higher flow rates than a conventional nasal cannula or nonrebreather mask, HFNC can more closely approximate the patient’s respiratory flow dynamics. HFNC can also provide CO2 washout of anatomic dead space and provide a small amount of positive end-expiratory pressure (PEEP), although that PEEP is drastically reduced when the patient’s mouth is open.7
Compared to conventional oxygen therapy, HFNC has been shown to reduce rates of endotracheal intubation8 in acute hypoxemic respiratory failure.9 Evidence is mixed when compared to NIV for preoxygenation for intubation,10 although the combination of HFNC and NIV appears to be better than either therapy alone.11 HFNC may be left in place during laryngoscopy to provide CO2 washout and apneic oxygenation and is likely better at preventing hypoxemia than conventional oxygen therapy.12
Pages: 1 2 3 4 | Single Page




No Responses to “Why the Nonrebreather Should be Abandoned”