
The Case Continues
After being discharged, the patient had an uneventful night. The next morning, he began to feel worse, and two days after the initial visit, he returned to the emergency department. His exam was now notable for “significant edema” at the left ankle, with bruising up the leg. Extreme tenderness was noted, but there was no crepitus.
Explore This Issue
ACEP Now: Vol 39 – No 12 – December 2020Vital signs were notable for slight tachycardia at 105 bpm, though his blood pressure, respirations, and pulse remained normal. His CBC and comprehensive metabolic panels were essentially unchanged (see Figure 3).
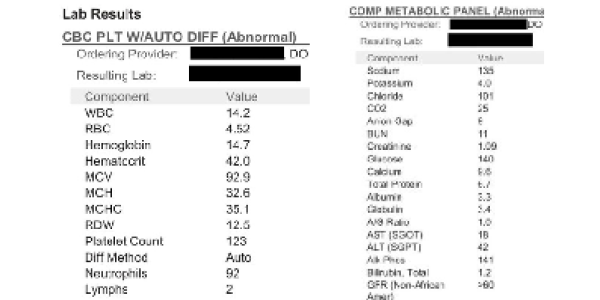
Figure 3
He was diagnosed with cellulitis and admitted to the hospital due to the severity of the swelling, bruising, and pain. The patient had a penicillin allergy listed and was started on vancomycin monotherapy. The emergency physician wrote a long note, including the reasoning shown below:
Consideration for necrotizing fasciitis was done however there is nothing on patient’s exam or history to assess that this is present. Patient’s had leg pain now for a couple of days and this has not been rapidly worsening the patient did state that it got significantly worse today. Pain is not out of proportion. Patient hasn’t had any significant fever and white blood cell count is not significantly elevated.
In the hospital, the patient developed renal failure, and his vitals worsened. A surgeon was consulted, and the patient was taken to the operating room. There was purulent drainage from the leg, and small areas of necrotic muscle were identified.
The patient was ultimately transferred to a larger medical center. He underwent several repeat operations for necrotizing fasciitis, ultimately requiring several skin grafts leading to permanent disability of his left leg.
The Lawsuit
The patient filed a lawsuit against the hospital. The plaintiff’s attorney alleged EMTALA violations, and therefore the lawsuit was filed in federal court. The specific claim was that the medical screening exam violated EMTALA because it did not lead to the correct diagnosis of necrotizing fasciitis.
The judge ultimately dismissed the lawsuit. In his opinion, he noted that “EMTALA is not a medical malpractice statute, and failing to correctly diagnose Plaintiff’s illness does not give rise to [EMTALA] liability.” This concept was reiterated throughout his opinion, and elsewhere he stated, “Defendants cannot incur EMTALA liability for what is merely an incorrect diagnosis.”
The patient proceeded to sue the hospital and all of the doctors involved in the case in state court. That lawsuit was eventually withdrawn without any mention of a settlement.
Pages: 1 2 3 | Single Page




No Responses to “What Is—and Isn’t—Guaranteed Under EMTALA Can Be Complex”