Whenever performing an ultrasound-guided nerve block, we recommend the patient be placed on continuous cardiac monitoring and pulse oximetry. Also, the operator should be aware of the possibility of local anesthetic systemic toxicity (LAST). The clinician should know the availability of 20% lipid emulsion therapy and dosing (lipidrescue.org).
Explore This Issue
ACEP Now: Vol 36 – No 03 – March 20172. Survey scan.
Moving acutely injured trauma patients is often not possible. In our experience, the following two patient positions have allowed for successful SAPB in all of our acutely injured patients.
Position 1: Lateral decubitus. Roll the patient in a lateral decubitus position (contralateral to the injury). If possible, ask the patient to place a hand behind the head.
Place a high-frequency linear transducer in the transverse plane (probe marker facing the nipple) at the level of the fifth rib (surface anatomy = approximately at the level of nipple) in the midaxillary line (see Figures 3A and 3B). Ultrasound landmarks that will be easily recognized by clinicians with some chest sonography experience include the hyperechoic ribs (anechoic shadow) and the pleural line. Find these basic landmarks first and then slowly attempt to locate the more superficial soft tissue structures. The serratus anterior muscle (flat and elongated) lies just superficial to the ribs, with the intercostal muscles deeper and in between the bony ribs. The latissimus dorsi muscle will be seen superior and posterior to the serratus anterior muscle and can act as a nice landmark (see Figures 4A and 4B and Figures 5A and 5B).
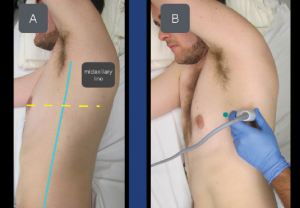
Figure 3A & B: To locate the serratus anterior muscle, place the transducer at the level of the nipple in the midaxillary line. The transducer marker (green dot) should point toward the nipple.
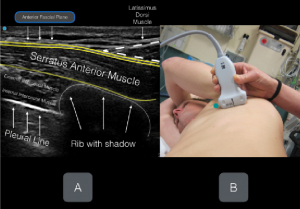
Figures 4A & B: Labeled ultrasound image with corresponding transducer positioning. Note the anterior fascial plane of the serratus anterior muscle. The goal of the planar block is to place anesthetic in this fascial plane.
In some patients, a slight clockwise rotation of the transducer will allow for an improved cross-sectional view of the ribs and the pleural line.
Position 2: Supine. The SAPB can be performed with the patient in a supine position as well and may be ideal in cases of multi-trauma or cervical spine injury or when the lateral decubitus position is not tolerated.
Place the transducer in the midaxillary line (probe marker facing the nipple) and locate the ribs (anechoic shadow), pleural line, and serratus anterior muscle (as above). The latissimus dorsi muscle may not be clearly visualized with the transducer in the more anterior position. Again, the fascial plane located on top of the serratus anterior muscle will be the target for anesthetic deposition.
Pages: 1 2 3 4 | Single Page




6 Responses to “Ultrasound-Guided Serratus Anterior Plane Block Can Help Avoid Opioid Use for Patients with Rib Fractures”
April 3, 2018
Santi Di PietroCongratulations for the article! Clear and complete… how should I cite it in a scientific research?
Sincerely
Santi Di Pietro
Junior EM Resident,
University of Pavia
April 9, 2018
Dawn Antoline-WangThe citation for this article is:
Nagdev A, Mantuani D, Durant E, Herring A. The ultrasound-guided serratus anterior plane block. ACEP Now. 2017;36(3):12-13.
August 14, 2018
Jonathan CheungIs this plane block effective as a one-off procedure or do you often need to repeat it later?
May 9, 2020
Dr.S.RadhakrishnaThank you for this useful article. The figure 2 shows the vertebra pointing in the wrong direction. The spinous process should point posteriorly and the body anteriorly. An error?
March 23, 2021
Dr Maya DehranThanks for sharing the very useful simple technique to treat the severe pain of chest injury.
January 18, 2022
DAVID CAMPELL, MDHow long does this block last before it has to be repeated to maintain pain control?