
Ethylene glycol (EG), also known as ethane-1,2-diol, with the molecular formula CH2OHCH2OH, is a colorless, odorless, water-soluble liquid commonly used as antifreeze fluid in automobile radiators, and remains an important cause of significant and sometimes fatal toxicity in the United States, with approximately 6,000 exposures and 20 deaths reported to poison centers in 2021.1 After possible exposures, early diagnosis and treatment are critical for preventing morbidity and mortality. However, the diagnosis of EG exposures continues to be problematic due to inconsistent history, restricted availability of EG-specific testing, and inconsistent time-sensitive indirect clues in laboratory analysis.
Explore This Issue
ACEP Now: Vol 42 – No 10 – October 2023Case
A young adult male with a prior history of self-harm presented 30 minutes after stating he “might have drunk half a gallon of antifreeze.” Physical examination revealed an awake, anxious-appearing, tachycardic man with no other abnormalities. Laboratory data were notable for normal renal function, osmol gap 24 (normal range, -14 to +10), anion gap 10 (normal range, 3 to 13), and normal urine without crystals. He was empirically loaded with fomepizole (15 mg/kg). The patient’s urine was obtained and compared with the urine of his emergency physician using a Wood’s lamp, and the patient’s was found to be brightly fluorescent, supporting the presumptive diagnosis of EG poisoning. After 12 hours, his initial EG level returned 130 mg/dL. After resolution of EG poisoning, he was transferred to psychiatry and ultimately discharged home without complication.
Discussion
The diagnosis of EG ingestion is problematic, often made on suggestive indirect information, and must be made quickly because time represents renal injury. The bedside physician must gather as many direct and indirect, classically suggestive data as possible and decide which are “bad” (they probably drank it), or “good” (they probably didn’t). The presence of urine fluorescence might be additive to this data collection.
History
Someone saw them drink the EG. This is bad (direct evidence). Their experience drinking the liquid. For example:
Doctor: “I bet it was terrible when you drank it, huh?”
Patient: “You know Doc, it wasn’t so bad, actually sort of sweet.”
This is bad (indirect evidence).
Laboratory Results
Osmol gap: If the gap is large—this is bad (indirect evidence). However, it is the parent alcohol that causes the gap, and with a typical half-life of three to six hours (peaking at 30 to 60 minutes) once it has been metabolized, the gap goes away.2 Additionally, there are large variations in the range of osmol gaps depending on the equation used to calculate osmolarity and the fact that some people naturally have negative osmol gaps. Because of this large range of values, small osmol gaps cannot be used to eliminate the possibility of toxic alcohol ingestion.3,4
Anion gap metabolic acidosis: if this is large—very bad (indirect evidence). The toxic metabolites of EG ingestions are what cause the acidosis (glycolic, glyoxylic, and oxalic acids as well as lactate) and present later in the ingestion after EG is metabolized to these bad actors. Once there is an anion gap, the horse has left the barn and the remaining definitive treatment is hemodialysis. Additionally, anion gap acidoses occur for other reasons (recall the mnemonic MUDPILES: methanol, uremia, diabetic or alcoholic ketoacidosis, paraldehyde, isoniazid, lactic acidosis, ethanol/ethylene glycol, or salicylates).
Urine crystals: presence of octahedral or needle-shaped calcium oxalate crystals in the urine—very bad (direct finding). The precipitation of oxalate crystals in the renal tubular lumen resulting in blockage is the primary cause of renal injury. Unfortunately, urinary crystal absence does not rule out EG ingestion.5
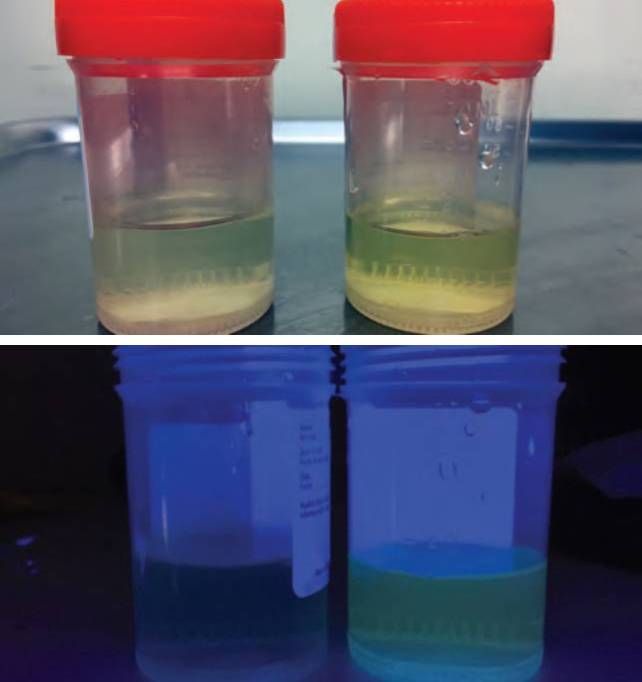
FIGURES 1A and 1B: Comparison of physician’s (LEFT) and patient’s urine (RIGHT) under normal light (TOP) and under Wood’s lamp (ABOVE) in urine cups. (Click to enlarge.)
Urine fluorescence: if the urine is fluorescent—very bad (direct finding). Sodium fluorescein (uranine yellow), is a fluorescent dye that is added to some commercial antifreeze preparations to assist in the location of engine coolant leaks. It is found in concentrations typically between 15 and 20 μg/mL.6 It causes a yellowish-green fluorescence that is visually detectable to a lower limit of 20 ng/mL in liquid when exposed to ultraviolet light.7
In medicine, the application of Wood’s lamp produces light photons in the ultraviolet light wavelength spectrum, in a range between 320 nm and 400 nm with a peak at 365 nm. When a substance absorbs light or energy (photons) from one source, its own photons get excited; when these excited photons relax they produce (emit) light of a different color. The re-emitted photons, or fluorescence, have no heat, a longer wavelength, lower energy, and a different color that disappears when the exciting light is removed. This light reaction is used in medicine for many purposes, including detection of dermatologic abnormalities in skin and nails by making them glow, such as dermatophytes (Tinea versicolor, etc.), bacterial infections (Pseudomonas, etc.) and porphyria (porphyria cutanea tarda, etc.). It is also used in ophthalmologic diagnostics of retinal vasculature imaging and corneal insult assessment. Other uses include detection of scorpions and semen. Urine may also fluoresce under this “blacklight” after ingestion of riboflavin and niacin, amoxicillin, and carbamazepine.8

FIGURES 2A and 2B: Patient’s urine under
normal light (TOP) and under Wood’s lamp
(ABOVE), demonstrating bright fluorescence
in urinal.
Research into urine fluorescence to help EG diagnosis has been both supportive and dismissive. Winter, et al., in 1990 showed nearly 100 percent detection after volunteer ingestion of fluoresceine at zero to two hours and 60 percent at four hours in volunteers.6 Other studies have shown poor detection and sensitivity of fluorescent presence in urine, false positives in children, and complication by fluorescence of the containers (some glass and plastic test tubes can glow), all of which may limit clinical use.9–11
In our case, despite having a markedly elevated EG level (130 mg/dL), the patient’s ED examination was normal; while his laboratory results were notable for elevated osmol gap (with no prior for comparison), he had normal renal function, no anion gap, urine that had no visual abnormality and no crystals. What he did have was brightly fluorescent urine—on its own and when compared with the bedside physician’s urine held in various identical containers (a urine cup, a urinal) and exposed to a Wood’s lamp. This information was considered in real time as supporting the presumptive diagnosis of EG ingestion and need for treatment.
Conclusion
Diagnosis of EG poisoned patients may be confounded by historical uncertainty, delayed return of definitive toxic alcohol levels, unreliable osmol gaps, and delayed development of other abnormalities. Although experimentally doubted, the detection of strongly positive fluorescent urine in the setting of a suspected recent ingestion of a fluorescein-containing EG product may bring additional support to initiation of therapy (before development of urinary crystals or an anion gap metabolic acidosis). The addition of a concurrent comparison with a control (even if your own) may also be useful. It may also be useful in resource-poor environments where laboratory testing is limited.
 Dr. Hack is chief of the division of medical toxicology and vice chair for research at East Carolina University in Greenville, North Carolina.
Dr. Hack is chief of the division of medical toxicology and vice chair for research at East Carolina University in Greenville, North Carolina.
References
- Gummin DD, Mowry JB, Beuhler MC, et al. 2021 annual report of the National Poison Data System (NPDS) from America’s poison centers: 39th annual report. Clin Toxicol (Phila). 60(12):1381-1643.
- Gessner PK, Parke DV, Williams RT. Studies in detoxication. 86. The metabolism of 14C-labelled ethylene glycol. Biochem J. 1961;79:482-489.
- Hoffman RS, Smilkstein MJ, Howland MA, et al. Osmol gaps revisited: normal values and limitations. J Toxicol Clin Toxicol. 1993;31(1):81-93.
- Takayesu JK, Bazari H, Linshaw MD. Case 7-2006: A 47-Year-Old Man with Altered Mental Status and Acute Renal Failure. N Engl J Med. 2006;354:1065-72.
- Boyer EW, Mejia M, Woolf A, et al. Severe ethylene glycol ingestion treated without hemodialysis. Pediatrics. 2001;107(1):172-3.
- Winter ML, et al. Urine fluorescence using a Woods lamp to detect the antifreeze additive sodium fluorescein: A qualitative adjunctive test in suspected ethylene glycol ingestions. Ann Emerg Med. 1990;19:663-667.
- O’Neil MJ. Merck Index. 13th ed. Whitehouse Station (NJ):Merck & Co;2001:736.
- Sharma S, Sharma, A. Robert Williams Wood: pioneer of invisible light. Photodermatol Photoimmunol Photomed. 2016;32:60-65.
- Wallace KL, Suchard JR, Curry SC, et al. Diagnostic use of physicians’ detection of urine fluorescence in a simulated ingestion of sodium fluorescein–containing antifreeze. Ann Emerg Med. 2001;38:49-54.
- Parsa T, Cunningham SJ, Wall SP, et al. The usefulness of urine fluorescence for suspected antifreeze ingestion in children. Am J Emerg Med. 2005;23:787–792.
- Casavant MJ, Shah MN, Battels R. Does fluorescent urine indicate antifreeze ingestion by children? Pediatrics. 2001;107(1):113-114.
Pages: 1 2 3 4 | Multi-Page




No Responses to “Toxicology Answer: An Illustrated Case of Ethylene Glycol, Direct and Indirect”