
I initiate the laryngeal handshake with my dominant right hand (see Figure 5). Ergonomically, I prefer to stand on the patient’s right side (at the thorax) so that when holding the scalpel, I can rest my cutting hand on the sternum. (We will address sternal stabilization in part two of this series.)
Explore This Issue
ACEP Now: Vol 33 – No 02 – February 2014I started gently up high with the hyoid, using the thumb and index finger, under the angle of the mandible. Staying lateral to midline, slide down to the broad, firm, thyroid lamina. At this point, use the index finger to come to midline and palpate the thyroid prominence in men. Lower down is the inferior cornu of the thyroid, bilaterally overlapping the cricoid cartilage. This is the bottom of the rhomboid, below which are the softer tracheal rings. Using the firm lamina of the thyroid as a guide (and especially if the thyroid prominence is not felt) the index finger is brought midline to the cricothyroid membrane at the inferior aspect of the lamina. In men, the thyroid cartilage is always more prominent than the cricoid, but in women they often have equal prominence.
After performing the laryngeal handshake with the dominant hand, switch to the non-dominant hand and grab the same landmarks. Use the non-dominant hand to stabilize the larynx (on the thyroid lamina) with the index finger over the cricothyroid. The dominant hand holds the scalpel and is stabilized on the sternum. Sternal stabilization is needed to make a controlled incision. We address this in part two of this series.
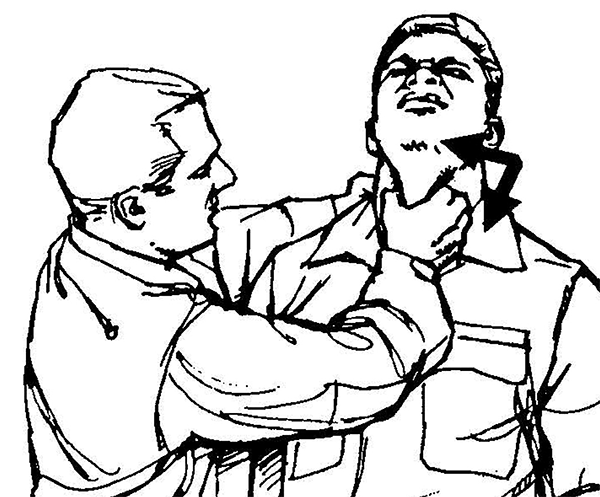
Figure 4.
An image from the US Army Field Manual of Close Quarters Combat showing the trachea choke; the laryngeal handshake is a gentle version of this five-finger palpation of the larynx, using a side-to-side motion to confirm palpation of the thyroid lamina.

Figure 5.
The laryngeal handshake, starting on right side with dominant hand (top), then switching to the nondominant hand on larynx, with the dominant hand getting ready to make the incision (bottom).
Pages: 1 2 3 | Single Page





6 Responses to “Tips and Tricks for Performing Cricothyrotomy”
February 10, 2015
Approaching the Awake Intubation - MarylandCCProject.org[…] “safely” in the risky zone. Welcome her to the resuscitation room with a gentle laryngeal handshake and be prepared to perform a surgical airway. Obviously, I have as much interest in performing […]
March 4, 2015
Approaching the Awake Intubation | Vinnie's ICU[…] think we’re “safely” in the risky zone. Welcome her to the resuscitation room with a gentle laryngeal handshake and be prepared to perform a surgical airway. Obviously, I have as much interest in performing […]
June 10, 2015
Approaching the Awake Intubation | University of Maryland[…] “safely” in the risky zone. Welcome her to the resuscitation room with a gentle laryngeal handshake and be prepared to perform a surgical airway. Obviously, I have as much interest in performing […]
August 25, 2015
Surgical airway training: technical and nontechnical skills and trainers | airwayNautics[…] that unanticipated difficult airways occur, always having a plan for failure and identifying the surgically inevitable airway early will help the team perform a surgical airway when it is required before too […]
September 10, 2015
Obesity Emergency Management | EM Cases : Emergency Medicine Cases[…] in obesity emergency management, Dr. Levitan recommends first identifying the midline using the laryngeal handshake technique or ‘rocking the rhomboid‘ and cutting a large vertical skin incision rather than first […]
May 4, 2018
emDOCs.net – Emergency Medicine EducationEM Cases: Obesity Emergency Management - emDOCs.net - Emergency Medicine Education[…] in obesity emergency management, Dr. Levitan recommends first identifying the midline using the laryngeal handshake technique or ‘rocking the rhomboid‘ and cutting a large vertical skin incision rather than first […]