
Ultrasound-guided nerve blocks (UGNBs) have become an integral part of emergency medicine practice, offering targeted analgesia while reducing reliance on opioids. Yet, in the rush to master anatomy, technique, and ultrasound visualization, clinicians may overlook the broader context of pain management. A nerve block should not exist in isolation; rather, it should function as one component of a structured, multimodal pain strategy that spans from patient arrival through disposition.1,2
Explore This Issue
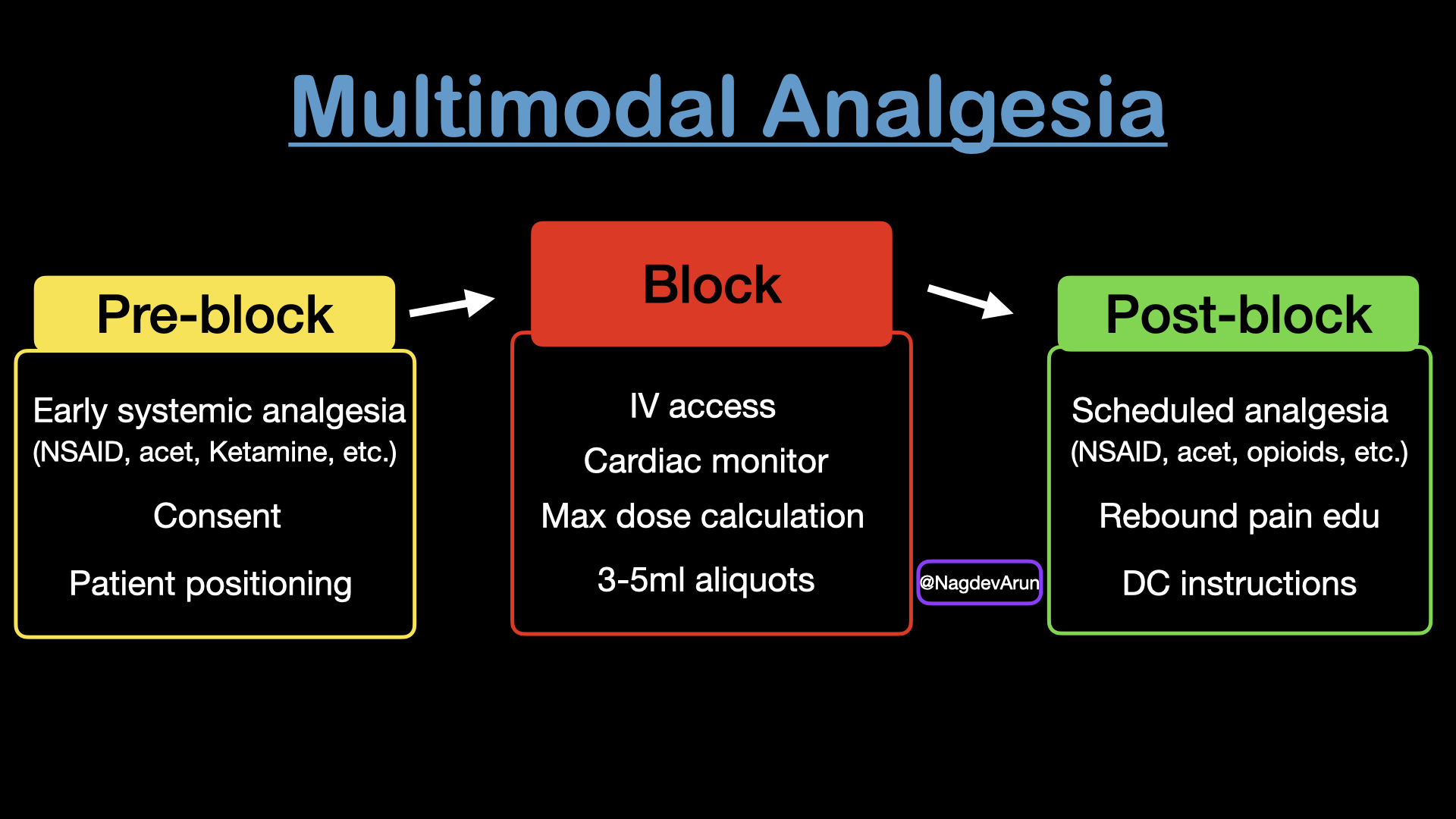
ACEP Now: March 2026We recommend approaching every block — and the patient’s overall pain control — through three deliberate phases:
Click to enlarge.
- Pre-block analgesia
- Intra-procedural safe anesthetic deposition
- Post-block pain planning
Thinking about pain across these stages allows clinicians to provide safe, durable analgesia while anticipating and addressing common pitfalls at each phase.
Pre-Block Analgesia: Foundational Pain Management
Optimal pain control begins well before the needle touches the skin. Patients in acute pain deserve early administration of systemic analgesics. When not contraindicated, acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) should be initiated promptly to reduce baseline discomfort and overall nociceptive input. In some cases, this early intervention may also reduce the anesthetic dose or volume required for effective blockade.
For patients with more severe pain, small doses of intravenous opioids or ketamine can improve comfort and facilitate positioning for the block. In our experience, ketamine 0.2–0.3 mg/kg diluted in 50 mL of normal saline and administered over 15 minutes is effective for reducing pain and procedure-related anxiety. This mirrors a familiar principle seen with lumbar punctures and other bedside procedures: early analgesia and anxiolysis often determine procedural success and patient satisfaction.3,4 patients scheduled for shoulder arthroscopy received ultrasoundguided single-shot Interscalene Brachial Plexus Block preoperatively and were randomized to receive either intravenous esketamine (0.5 mg/kg bolus + 0.25 mg/ kg/h infusion).
Finally, informed consent should include a brief explanation of the block’s purpose, expected duration, and potential risks. The clinician should clarify that the goal is multimodal pain control and not surgical anesthesia. This helps align expectations and reassure patients before the procedure.
Intra-Procedural Management: Precision and Safety
During the procedure, the clinician’s focus shifts to technical execution and patient safety. Patients undergoing blocks that require larger anesthetic volumes (generally >10–15 mL) or are performed near vascular structures should have intravenous access and continuous cardiac monitoring, maintained during the procedure and for approximately 30 minutes afterward.
The maximum safe anesthetic dose should be calculated in advance, particularly when using long-acting agents such as bupivacaine or ropivacaine. We recommend using an anesthetic dosing calculator or electronic health record-embedded tools to minimize dosing errors.
After skin wheal placement and needle entry, the goal is continuous visualization of the needle tip as it is advanced toward the target nerve or fascial plane. In our practice, small volumes of normal saline are frequently used for hydrolocation (to confirm needle tip position) and hydrodissection (to open appropriate fascial planes). Once the ideal location is achieved, anesthetic should be injected in 3–5 mL aliquots, with pauses between injections to confirm negative aspiration and reassess the patient for early signs of local anesthetic systemic toxicity. Maintaining needle tip visualization under ultrasound guidance remains the most effective method to prevent inadvertent intravascular or intraneural injection.5
For higher-volume blocks — such as the serratus anterior plane block or erector spinae plane block — additional time between aliquots is warranted. Clinicians should monitor closely for changes in heart rate, blood pressure, or mental status. In our experience, slowing the injection process not only improves safety but also reduces operator stress during these procedures.
Post-Block Pain Planning: Completing the Arc
The post-block phase is often underappreciated, yet it is critical to long-term analgesic success. As the block wears off, patients may experience abrupt and severe pain—commonly referred to as rebound pain. Although the precise mechanism and evidence base remain incompletely defined, this phenomenon is well recognized and should be anticipated whenever a single-injection nerve block is performed.
Clinicians should establish a clear post-block medication strategy for all patients receiving single-shot UGNBs. We recommend a scheduled multimodal analgesia regimen (for discharged and admitted patients) for the first 24 hours following the block. In our experience, “as needed” dosing should be discouraged, because patients frequently decline analgesics while the block is effective, and request medication only after the block is starting to wear off. The resultant increased pain can be extremely distressing and very difficult to control.
Patient and staff education is essential. A multimodal regimen incorporating NSAIDs, acetaminophen, and, when appropriate, short-course opioids can significantly reduce the severity of rebound pain. After the initial 24-hour period, patients can taper medications as tolerated. Clear written instructions and discharge counseling should accompany all outpatient blocks.6
Although continuous peripheral nerve catheters may mitigate rebound pain, they are not commonly used in the ED setting due to logistical and follow-up limitations. As such, thoughtful post-block planning remains essential for single-shot techniques.
With this article, Dr. Nagdev shares his final Sound Advice column for ACEP Now and his thoughts on the practice below. ACEP Now thanks him for his contributions.
Dr. Nagdev
It has been a privilege to write about point-of-care ultrasound (POCUS) for ACEP Now’s Sound Advice, and in particular to introduce and expand the conversation around ultrasound- guided regional analgesia for emergency clinicians. In my opinion, POCUS has become a critical imaging modality for all emergency physicians and continues to grow rapidly beyond the ED into nearly every area of medicine. As the field evolves, having new authors bring fresh perspectives on how we teach, apply, and integrate POCUS is essential to the continued growth of Sound Advice. POCUS is the future of medicine, and I look forward to reading the outstanding work ahead in the years to come.
Thanks,
Arun
Implementing a holistic approach to nerve blocks does not require a complex protocol—it requires a mindset. Each block should be viewed as one pillar of a broader, patient-centered analgesic strategy. In practice, this means:
- Initiating multimodal analgesia early, before performing the UGNB
- Performing the block safely, with appropriate dosing and continuous ultrasound visualization
- Planning proactively for rebound pain, with a documented and communicated post-block regimen
As UGNBs become increasingly routine in emergency care, this approach can help standardize practice and improve pain outcomes for patients with acute injuries.
Summary: The Block Is Just the Beginning
Ultrasound-guided nerve blocks are among the most powerful tools available for acute pain management in the emergency department. However, procedural expertise alone is insufficient. Developing a comprehensive analgesic plan, from early systemic pain control to precise block performance to intentional post-block care, enhances both block efficacy and the patient experience. By thinking holistically about the lifecycle of a nerve block, we move beyond procedural success toward comprehensive, patient-centered pain care. The result is safer, more compassionate, and more durable analgesia for the patients we serve.
Dr. Nagdev is the Emergency Ultrasound Division Director, Alameda Health System – Highland Hospital.
Dr. Martin is the Emergency Ultrasound Fellowship Director, Alameda Health System – Highland Hospital.
Dr. Stegeman is the Community Ultrasound Director, Alameda Health System – Highland Hospital.
Dr. Brown is Associate Program Director at Denver Health Emergency Medicine and Education Director, Point-of-Care Ultrasound Group at the University of Colorado, Anschutz Medical Campus.
Dr. Goldsmith is Vice-Chair of the Department of Emergency Medicine at Lahey Hospital at the University of Massachusetts-Chan Lahey School of Medicine.
References
- Goldsmith AJ, Brown J, Duggan NM, et al. Ultrasound-guided nerve blocks in emergency medicine practice: 2022 updates. Am J Emerg Med. 2024;78:112-119.
- Lee JS, Chenkin J, Simard R, et al. Ultrasound-Guided Regional Anesthesia by Emergency Physicians for Hip Fractures and Delirium: A Randomized Clinical Trial. JAMA Netw Open. 2025;8(12):e2549337.
- Chen J, Pan Z, Zheng J. Effect of Intravenous Esketamine on Rebound Pain Following Single-Shot Brachial Plexus Block in Patients Undergoing Shoulder Arthroscopic Surgery: A Prospective, Randomized, Placebo-Controlled Study. J Pain Res. 2025;Volume 18:5235-5248.
- Khan Z, Hameed M, Khan FA. Current role of perioperative intravenous ketamine: a narrative review. Anesthesiol Perioper Sci. 2023;1(4):36.
- Driver L, Perice L, Brown JR, Nagdev A, Goldsmith A. Ultrasound-guided nerve blocks: expert opinion statement on patient monitoring in the emergency department setting. Intern Emerg Med. 2025;20(8):2589-2591.
- Brown J, Goldsmith A, Duggan N, Stone A, Nagdev A. Ultrasound-guided nerve blocks: discharge guidelines. Intern Emerg Med. Published online November 14, 2025.




No Responses to “Take a Holistic Approach to Ultrasound-Guided Nerve Blocks”