
Case
A 64-year-old man has a witnessed out-of-hospital cardiac arrest (OHCA) while attending a hockey game. Bystander CPR is immediately started while an automatic external defibrillator (AED) is located. He is found to be in ventricular fibrillation and receives two defibrillation attempts with the AED. Emergency Medical Services (EMS) arrive and provide another defibrillation with their machine, but the patient remains in refractory ventricular fibrillation.
Explore This Issue
ACEP Now: Vol 42 – No 04 – April 2023Clinical Question: In patients with refractory ventricular fibrillation, does vector change (VC) of the pads or double sequential external defibrillation (DSED) work?
Background: Multiple different therapies have been tried to improve the survival of OHCA patients. This has included therapeutic hypothermia, supraglottic devices, crowd sourcing CPR and epinephrine.1–4 A couple of issues that have not been looked at is pad placement and double sequential external defibrillation.
Reference: Cheskes S, Verbeek PR, Drennan IR, et al. Defibrillation strategies for refractory ventricular fibrillation. N Engl J Med. 2022;387(21):1947–1956.
- Population: Adult patients (18 years of age or older) and had an OHCA and refractory ventricular fibrillation (three standard shocks).
- Intervention:
- Vector Change Defibrillation: Pads are placed in an anterior-posterior pad placement after standard anterior-anterior configuration following the third shock.
- Double Sequential External Defibrillation: Pads are placed in both the anterior-anterior and the anterior-posterior pad placements following the third shock with standard defibrillation.
- Comparison: Standard defibrillation with pads placed in anterior-anterior configuration
- Outcome:
- Primary Outcome: Survival to hospital discharge
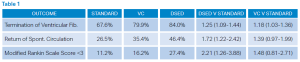
- Secondary Outcomes: Termination of ventricular fibrillation, return of spontaneous circulation (ROSC), good Neurologic outcome (modified Rankin scale [mRS] score less than three)
Authors’ Conclusions: “Among patients with refractory ventricular fibrillation, survival to hospital discharge occurred more frequently among those who received DSED defibrillation or VC defibrillation then among those who received standard defibrillation.”
Click to enlarge.
Results: They enrolled 405 patients into the study. The mean age was 64 years, over 84 percent were male, 68 percent were witnessed arrests, 58 percent had bystander CPR performed, and median response time was eight minutes.
Key Result: Survival was greater in those patients who had vector change or double sequence defibrillation compared to standard treatment.
- Primary Outcome: Survival to hospital discharge
- Vector Change vs standard group 21.7 percent versus 13.3 percent; relative risk 1.71 (95 percent CI, 1.01 to 2.88).
- DSED 30.4 percent versus standard 13.3 percent; relative risk 2.21 (95 percent CI, 1.33 to 3.67)
- Secondary Outcomes: DSED but not VC defibrillation was associated with a higher percentage of patients having a good neurologic outcome than standard defibrillation (relative risk 2.21 [95 percent CI, 1.26 to 3.88] and 1.48 [95 percent CI, 0.81 to 2.71] respectively)
EBM Commentary
- Blinding—This was a double blinded study. The patients and outcome assessors were unaware of group allocation while the treating paramedics were aware of the assigned defibrillation strategy. It is unclear what would have biased the primary outcome of survival to hospital discharge.
- Cluster Randomized Control Trials—There is a difference between individual RCTs and cluster randomized trials. Cluster randomization means you cluster groups of individuals as a unit making the number of independent units allocated smaller than the actual number of observations. There are some advantages and disadvantages to performing cluster RCTs.5
- Stopping Early—Stopping a trial early can introduce potential bias into a trial.6–8 Some of these biases can be mitigated by deciding a priori what conditions would result in halting the trial. This trial, like many others, was stopped due to COVID. They were only able to get 44 percent of their planned sample size.
SGEM Bottom Line
Consider changing your vector or doing double sequential external defibrillation in patients with refractory ventricular fibrillation.
Case Resolution
The EMS paramedics add their defibrillator with pads in the anterior-posterior position and provide DSED. The patient is successfully defibrillated and transported to the local emergency department.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.
Thank you to Dr. Seam Moore, an emergency physician working in Kenora, Ontario, for his help with this review.
 Dr. Milne is chief of emergency medicine and chief of staff at South Huron Hospital, Ontario, Canada. He is on the Best Evidence in Emergency Medicine faculty and is creator of the knowledge translation project The Skeptics’ Guide to Emergency Medicine.
Dr. Milne is chief of emergency medicine and chief of staff at South Huron Hospital, Ontario, Canada. He is on the Best Evidence in Emergency Medicine faculty and is creator of the knowledge translation project The Skeptics’ Guide to Emergency Medicine.
References
- Dankiewicz J, Cronberg T, Lilja G, et al. Hypothermia versus normothermia after out-of-hospital cardiac arrest. N Engl J Med. 2021;384(24):2283–2294.
- Benger JR, Kirby K, Black S, et al. Effect of a strategy of a supraglottic airway device vs tracheal intubation during out-of-hospital cardiac arrest on functional outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA. 2018;320(8):779–791.
- Ringh M, Rosenqvist M, Hollenberg J, et al. Mobile-phone dispatch of laypersons for CPR in out-of-hospital cardiac arrest. N Engl J Med. 2015;372(24):2316–25.
- Perkins GD, Ji C, Deakin CD, et al. A randomized trial of epinephrine in out-of-hospital cardiac arrest. N Engl J Med. 2018;379(8):711–721.
- Taljaard, Monica & Grimshaw, Jeremy. (2014). Concept, characteristics and implications of cluster randomization. Clinical Investigation. 4. 1–4.
- Lievre M, Menard J, Bruckert E, et al. Premature discontinuation of clinical trial for reasons not related to efficacy, safety, or feasibility. BMJ. 2001;322: 603–5.
- Bassler D, Matthias, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303: 1180–1187.
- Guyatt, GH, Briel, M, Glasziou, P, et al. Problems of stopping trials early. BMJ. 2012; 344.
Pages: 1 2 | Multi-Page




No Responses to “Study Compares Standard, Vector Change and Double Sequential Defibrillation”