One of the unforeseen changes to emergency medicine in the peri-pandemic era is the extreme variation in volume and acuity. Prior to the COVID-19 pandemic, it was not unusual to observe up to 15 percent variation in volume between the busiest and slowest days of the week. For instance, an emergency department might see 98 patients on Saturday and 113 patients on Monday. Acuity as measured by admission rate and Emergency Severity Index (ESI) distribution showed a similar degree of variation. Innovative department leaders understood these data and used them to optimize operations. By knowing the arrivals by day of the week and by hour of the day, stratified by the acuity of the patients presenting, medical directors can craft good baseline operational strategies. In particular, these data should inform the opening and closing of specific zones within an emergency department and optimize staffing patterns. For instance, many departments staff down on weekends and up on Mondays. Zone opening and closing times may vary by day of the week. Some emergency departments close the fast track on weekends for lack of patients to populate it. Communities with seasonal variation in population, such as emergency departments near vacation destinations, should also look at data by month.
Explore This Issue
ACEP Now: Vol 40 – No 10 – October 2021Since the pandemic, this variation has become extreme for many emergency departments. Some now report variation in daily volume of more than 40 percent, and the weekly patterns are now more difficult to identify. An emergency department such as the example mentioned above might now see 88 on the slowest day of the week and 127 on the busiest day. Even more confounding, the old weekend-to-Monday pattern may no longer apply. Many departments are seeing swings in the ESI distribution, such as steep drop-offs in volumes of low-acuity patients and upticks in high-acuity patient volume when COVID surges are prevalent in the community.
Factoring in the escalating phenomenon of staff callouts, this daily variability becomes even more problematic. Staff nurses have higher rates of callouts (absenteeism) than many other types of workers.1 Particularly in unionized workforces (where the “sick day” is viewed as a right and is protected), callouts are common. But COVID had impacted absenteeism even more, and now physicians and advanced practice professionals (APPs) are affected as well.2 Hospital leaders and managers are struggling to find remedies for an entire workforce that is burnt out, sick, or anxious about getting sick and so chooses to call out for a shift. Even physician groups are having to plan for doctors who call out. Nurse leaders and managers may spend the first part of a workday addressing callouts and trying to fill holes in the schedule.
What are some of the options for ED leaders trying to function with so much daily variation?
Flexible Geography
Since your peri-pandemic emergency department will need to be a different emergency department on any given day, with volume and acuity swings that are extreme, you need to think about how to accommodate the variation within the physical space.
- Flex Unit: A combined unit that can flex with the acuity distribution is an idea whose time has come. Here are a few examples of flex units:
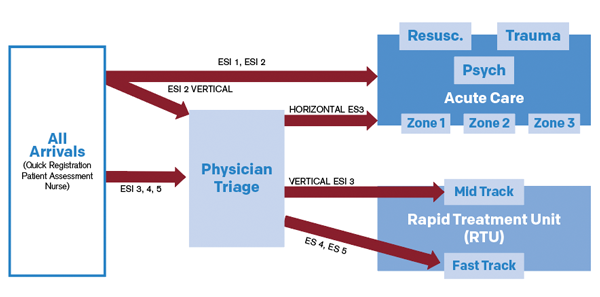
- Perhaps the most common example is the rapid treatment unit idea. The Tennity Emergency Department at Eisenhower Health in Rancho Mirage, California, designed a space that combines the fast track and the mid track (see Figure 1). Middle- and lower-acuity volumes showed the most variation in the peri-pandemic months, so this space was ideal for them, and patients were treated predominantly in recliners in this area. APPs saw the low-acuity patients and helped with some easier mid-track patients, who were predominantly managed by physicians. (See the February 2021 issue of ACEP Now for more on Tennity’s flexible ED design.)
- Conversely, an ED patient care area can be flexed into a boarding unit. At the Christiana Care emergency department in Wilmington, Delaware, a dual-purpose 11-bed “core” was identified as a flex zone. This area could be a lower-acuity zone, boarding unit, or hybrid unit based on the conditions of the day. An APP managed both groups of patients, and staffing was flexed accordingly. If this pod was used primarily for boarding and no new patients could be processed there, physician hours were saved by sending the clinician home.
- At Hasbro Children’s Hospital in Providence, Rhode Island, variation in both orthopedic surges and behavioral health surges were noted. Orthopedic cases peak in the summer, while behavioral health cases peak when school starts through the winter. The hospital has a zone that functions alternatively as an orthopedic suite or behavioral health holding suite based on the patient numbers each day. (See the March 2018 issue of ACEP Now for more on Hasbro Children’s Hospital’s efforts to improve metrics.)
- Flex Beds: A variation of the flexible geography concept is to identify flex beds or treatment spaces with proximity to a zone. This patient-centered approach was used at Washington Hospital Healthcare System in Fremont, California, in its new emergency department. It also helps when two clinicians have vastly different productivity and efficiency levels. This model allows each to work at their own pace by giving the clinicians more rooms to see patients when they can and fewer rooms when they can’t see the next new patient quickly. Figure 2 depicts two zones and a group of shared beds that can be part of either zone. (See the March 2019 issue of ACEP Now for more on Washington Hospital’s approach to moving to a larger ED space.)

Figure 2: With the flex-bed concept, two zones share
a group of flexible beds that can be part of either zone.
Flexible Shifts
Volume swings of 40 percent will always need adjustments in staffing. Helen DeVos Children’s Hospital in Grand Rapids, Michigan, created a model of flexibility in scheduling. Its shifts match the patient arrivals, not physician or nursing preference. The physicians have flexible shifts called “at-risk shifts.” These flex shifts may be four, eight, or 12 hours, depending upon departmental conditions. A real-time huddle of physician and nurse leaders is held to decide the strategy for opening and closing of zones in real time. Predetermined rules decide if and when the clinician goes home. They have well-articulated processes for most contingencies. (See the July 2019 issue of ACEP Now for more on Helen DeVos’s data-driven ED flow.)
On-Call Strategies
While most emergency physicians were attracted to the specialty because of the carefully delineated work hours, we may start needing an on-call arrangement. This will likely be a result of surges and the new extremes of volume variation. This may contribute to the need for on-call backup. Hospital leadership should articulate triggers for both calling in and sending home physicians and APPs. Real-time data should inform these triggers, which will be location specific. A few examples of triggers are listed below:
- Calling in a physician or nurse
- More than six people waiting in the waiting room
- More than 30-minute waits to see the clinician
- A sick clinician
- Sending a physician or nurse home
- Fewer than two arrivals per hour for a zone
- No nurse or tech to support the clinician
- Zone closure
The most progressive emergency departments are learning to build flex into their operations. Ideally, emergency departments should have these flex options mapped out beforehand and standardized to avoid confusion. In the emergency department, we are known for being very creative (anyone remember using a Foley catheter for a posterior nosebleed?), but inventing operations on the spot will be less successful than deliberately gathering your team together to brainstorm how to create more flexibility to manage the inevitable variability in your emergency department. Map out these plans, educate staff, and achieve buy-in in advance. By flexing your geography and your shifts and by planning for contingencies with on-call strategies, your emergency department will be able to bend without breaking as the situation around it changes.
References
- Pedder H, Jones T, Rejon CS. COV.12: impacts of absenteeism in doctors and nurses in primary care and community care. National Institute for Health Research website. Accessed Sept. 24, 2021.
- Kanwal N, Riaz G, Riaz MS, et al. Identify the causes of absenteeism in nurses Mayo Hospital Lahore Pakistan. Int J Soc Sc Manage. 2017;4(2):110-114.
Pages: 1 2 3 | Multi-Page




No Responses to “Strategies To Help Your ED Adapt to Variable Volumes and Patient Needs”