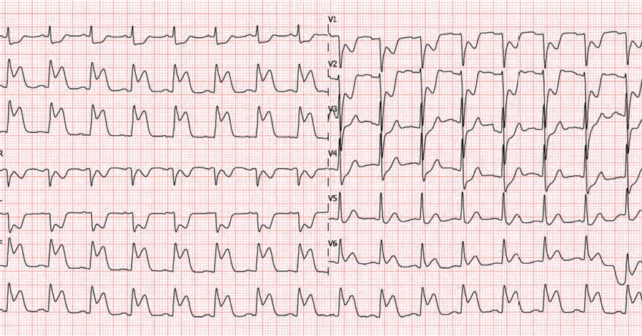
A 64-year-old male collapses after shovelling snow. Paramedics find a patient with eight out of 10 chest pain looking visibly uncomfortable. Vital signs are normal, but the ECG shows ST elevation in the inferior leads and some ST changes in V1-V2 that make you wonder if your patient is having an acute myocardial infarction (MI) with right-sided ventricular involvement (RVMI). In the emergency department, you administer 160 mg of chewable aspirin and your colleague asks if you should also administer 400 ug of nitroglycerin.
Explore This Issue
ACEP Now: Vol 43 – No 03 – March 2024Background
Many of us may have been taught not to give nitrates to a patient with an RVMI. This likely comes from the American Heart Association (AHA) guideline recommendation stating that nitroglycerin is contraindicated in these situations.1 It is categorized as Class III, LOE C (very low-level evidence) but has become part of clinical practice and EMS protocols.
The pathophysiologic rationale was that nitrates would cause vasodilation and thus reduce right ventricular preload, decreasing left end diastolic volume, and ultimately resulting in clinically important hypotension. Many times, pathophysiology has been used to explain something in medicine only to be discovered later that the human body is much more complex than we thought.
The evidence for this recommendation comes from a single retrospective observational study of 40 patients with inferior MIs published in 1989.2 A large portion, 20 patients (50 percent), had hypotension after being administered nitrates. Those with inferior MI and hypotension had ECG evidence of RV involvement. It is important to note that there was no standardization of the nitrate dose or route of administration, so it’s hard to know how to extrapolate the findings to our modern practice and protocols.
Clinical Question
In patients with right ventricular myocardial infarction (RVMI), is nitrate administration associated with increased adverse events compared to patients with myocardial infarctions in other anatomic regions?
Reference: Wilkinson-Stokes M, Betson J, Sawyer S. Adverse events from nitrate administration during right ventricular myocardial infarction: A systematic review and meta-analysis. Emergency Medicine Journal. 2022;40(2):108-13.
- Population: Adult patients diagnosed with an acute MI
- Exclusions: Patients with coronary vasospasm
- Exposure: Nitrate administration in any dose and by any route.
- Comparison: Patients with acute right-sided myocardial infarctions to patients with acute MI involving any other anatomic regions
- Outcome:
- Primary Outcome: Any adverse outcomes reported in the identified literature.
- The primary meta-analysis excluded studies of low quality, but a secondary analysis was also performed including identified studies (2) that were deemed of lower methodologic quality.
Authors’ Conclusions
“This review suggests that the [American Heart Association] and [European Society of Cardiology] contraindications [stating that nitrates are contraindicated in RV MI] are not supported by evidence. Key limitations include all studies having concomitant inferior and RVMI, no evaluation of beneficial effects in any of the studies, and very low certainty of evidence. As adverse events such as hypotension are transient and easily managed, nitrates are a reasonable treatment modality to consider during RVMI on current evidence.”
Pages: 1 2 3 | Single Page



2 Responses to “Revisiting Nitroglycerin in MI with Right-Side Ventricular Involvement”
March 10, 2024
Joseph Shiber, MDYou have missed the big picture. NTG will cause venodilation in every patient. If they are dependent on RV filling for contraction as during myocardial ischemia/infarction then you will expect this effect to be pronounced. It’s not that you can’t give NTG for the anti-anginal effect of potentially pain relief (that’s all the benefit you will ever get from NTG unless there is actual coronary artery spasm w/o complete coronary occlusion/thrombosis) but you need to be ready to intervene by stopping the NTG (it should be IV and not SL or topical since you need the effect to go away quickly) and give an IVF bolus. If you give a SL NTG and do not have IV access yet to give an IVF bolus, you will never forget this mistake even if the patient hopefully doesn’t arrest.
March 10, 2024
Andrew SchareAnother question to ask is why do we give nitrates at all to patients with acute myocardial infarction. There is no benefit to morbidity or mortality.