
Explore This Issue
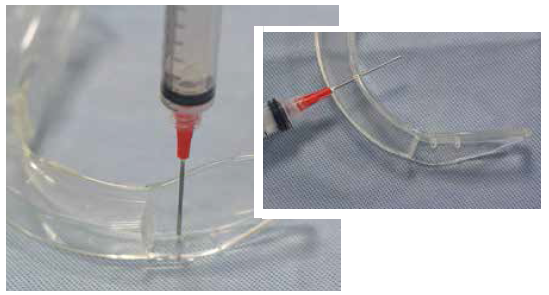
ACEP Now: Vol 34 – No 02 – February 2015Figure 4. Use the syringe to make three holes in the laryngoscope blade.
intubation. This novel apparatus will take approximately 20 minutes to assemble, so it should be put together prior to when it is needed. You can assemble it during your next night shift at 3:30 am and store it with your airway supplies. While the example below is applied to the GlideScope, this principle and assembly can also be applied to most other video laryngoscopes (eg, Karl Storz C-MAC).
Equipment Needed (see Figure 1)
- 10 cc syringe with 18 g blunt-tip needle
- One set of IV tubing
- Scissors
- Tape
- 0-0 silk suture
- Normal saline flush
- GlideScope disposable laryngoscope blade
- One needleless luer lock
Assembly
1. Cut the IV tubing as shown in Figure 2. Cut the distal end of the IV tubing at an oblique angle and fit the luer lock into the oblique opening. This may be take some elbow grease, but it will fit (Figure 3).
2. Use a 10 cc syringe with the 18 g needle as a drill and make the three individual holes as outlined in Figure 4.
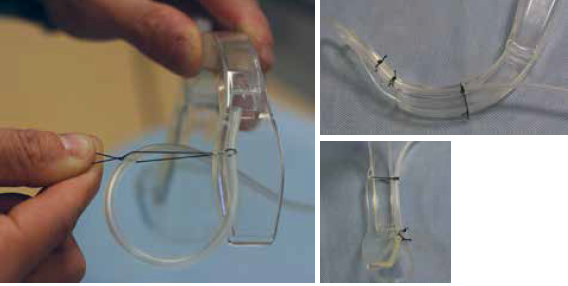
Figure 5. Fasten the IV tubing to the laryngoscope blade with 0-0 silk with the knot tied on the lateral aspect of the laryngoscope.
3. Fasten the IV tubing to the laryngoscope blade with 0-0 silk with the knot tied on the lateral aspect of the laryngoscope, avoiding any further obstruction of the GlideScope view (Figure 5). The end of the IV tubing should be secured in the corner of the laryngoscope blade within 0.5 cm of the lens. Additional holes can be made to further secure the IV tubing if needed.

Figure 6. Attach the remainder of the IV tubing to laryngoscope blade with tape.
4. The remainder of the IV tubing can be attached to laryngoscope blade with tape (Figure 6).
Utilization
1. The same technique for any GlideScope intubation is used with this apparatus: entering the oropharynx midline, rotating the blade, and visualizing the glottis.
2. If the lens becomes obscured by bodily fluid during the intubation, the operator or assistant can push 5 mL increments of normal saline through the IV tubing to clean the lens (Figure 7). This can be repeated as many times as needed to obtain a clear view and intubate the patient (Figure 8).
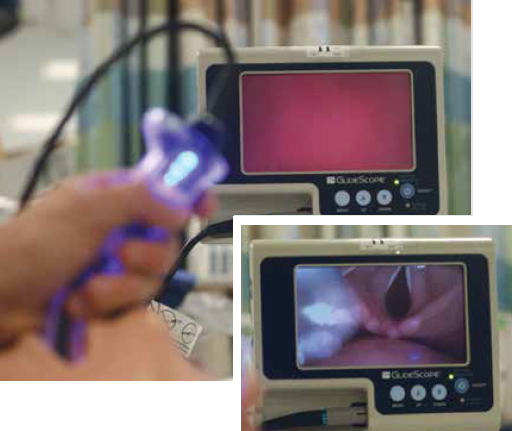
Figure 7. Push 5 mL increments of normal saline through the IV tubing to clean the lens.
Patient Selection
This apparatus could arguably be used with any intubation for which you are using video laryngoscopy. Our current bedside difficult-airway prediction tools are limited at best, and the rate of unexpected difficult airways has been shown to be as high as 52 percent even in controlled anesthesia settings.5,6 The most obvious patients who can benefit from this tool are those who are bubbling, bloody, or blowing chunks. In other words, patients who have significant bubbling pulmonary edema, have a traumatic bloody airway, or are actively vomiting (ie, blowing chunks), all of which could obscure the video
Pages: 1 2 3 | Single Page






2 Responses to “Keep Video Laryngoscope Clear with IV Tubing, Saline, and Some Ingenuity”
March 9, 2015
Kyle StevensWould love to see video of this DYI setup and of it in action
August 30, 2025
Frankfor hands free use:
attach a one way valve to an extension tubing. cut the other end of the extension tubing to length and fasten it to the blade as described. store it with your airway supplies.
To use the system connect a 100ml saline soft bottle to a regular iv tubing. connect the open end of the iv tubing to the one way valve on the blade. put the bottle on the ground, regulate the saline flow by pressing down your foot on the soft bottle.