The Case
A 52-year-old woman presents to the emergency department with sudden onset of palpitations and presyncope starting one hour ago. There has been no chest pain or shortness of breath. Examination is normal other than an irregularly irregular heart rate of 150 beats per minute. The patient’s past medical history is significant for gastroesophageal reflex disease for which she takes a proton pump inhibitor. The ECG shows classic atrial fibrillation with a rapid ventricular response.
Explore This Issue
ACEP Now: Vol 38 – No 11 – November 2019Background
Atrial fibrillation is the most common significant dysrhythmia in the emergency department.1 For decades, experts have debated whether a rhythm control or rate control strategy is best (eg, RAte Control versus Electrical cardioversion for atrial fibrillation [RACE] and Atrial Fibrillation Follow-up Investigation of Rhythm Management [AFFIRM]).2,3 The American College of Cardiology/American Heart Association/Heart Rhythm Society 2014 guidelines contain recommendations on the management of patients with atrial fibrillation.4
Practice variation in management of patients with atrial fibrillation has been noted. Physicians in the United Kingdom and Australia use rhythm control approximately half the time, while American physicians employ rhythm control one-quarter of the time.5
In Canada, the proportion undergoing rhythm control ranges from 42 to 85 percent. Even once rhythm control is selected, practice management varies. A chemical-first rhythm control approach is used in 56 percent of patients, while an electrical-first approach is used in 44 percent of patients.6
Clinical Question
In patients with acute uncomplicated atrial fibrillation, is sinus rhythm achieved faster with chemical-first or electrical-first rhythm control?
Reference: Scheuermeyer FX, Andolfatto G, Christenson J, et al. A multicenter randomized trial to evaluate a chemical-first or electrical-first cardioversion strategy for patients with uncomplicated acute atrial fibrillation. Acad Emerg Med. 2019;26(9):969-981.
- Population: Patients ages 18 to 75 years with atrial fibrillation of less than 48 hours duration with a CHADS2 score <2 (see Table 1).
- Excluded: Hemodynamic instability, atrial flutter, CHADS2 score ≥2, acute underlying medical illness, recent cardiac procedure, acute intoxication, or withdrawal from alcohol or illicit substances. Other excluded patients included those who came to the emergency department for other reasons (eg, trauma, gout) who were incidentally found to have atrial fibrillation.
- Intervention: Chemical-first rhythm control using IV procainamide followed by electrical cardioversion (if chemical cardioversion was unsuccessful).
- Comparison: Electrical-first rhythm control using a synchronized biphasic waveform sequence of 100J to 150J to 200J, with a maximum of three attempts, followed by chemical cardioversion with procainamide (if electrical cardioversion was unsuccessful).
- Outcome:
- Primary Outcome: Discharge within four hours of ED arrival.
- Secondary Outcomes: Additional median time intervals, ED-based adverse events, and 30-day patient-centered outcomes.
Authors’ Conclusions
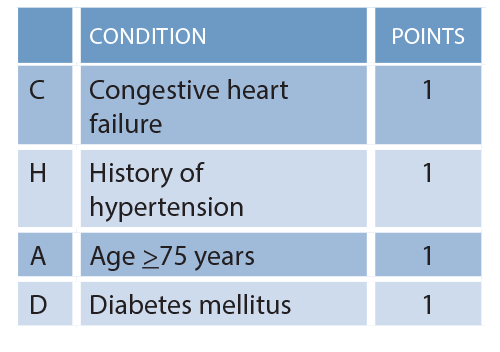
Table 1: CHADS2 Calculation
“In uncomplicated ED [atrial fibrillation] patients, chemical-first and electrical-first strategies both appear to be successful and well tolerated; however, an electrical-first strategy results in a significantly shorter ED length of stay. Our results should encourage clinicians to initially consider an electrical-first approach for such patients.”
Pages: 1 2 3 | Single Page




No Responses to “In Uncomplicated AFib, Is Electrical or Chemical Rhythm Control Best?”