
In the emergency department (ED), care for patients with substance use disorders, and in particular, those with opioid use disorder (OUD), is limited by numerous factors: inadequate clinician education, interpersonal stigma, insufficient social services support infrastructure, competing priorities, and high utilization.1-4 Intuitively, interventions aimed at improving access to care for this population benefit patients by increased retention in outpatient care, lowered frequency of harmful substance use, decreased transmission of infectious disease, and even reductions in morbidity and mortality.5-6 These interventions can also benefit ED clinicians and health systems through improved connectivity with outpatient follow-up, decreased ED return rates and hospital readmissions, and, in turn, potential cost savings.7
Explore This Issue
ACEP Now: February 2026 (Digital)However, care for patients with OUD is multidisciplinary, extending outside of the ED. These patients are cared for in every department, ranging from cardiothoracic surgery to psychiatry and every care setting, from outpatient clinics to hospital wards to the ED. Access to addiction-trained subspecialists through consult services remains limited.8 Taken together, interventions focused on caring for patients with OUD can be decentralized, without a clear stakeholder leading or “owning” this important work. This raises the question: How can emergency clinicians involve themselves in interventions that aim to improve outcomes for this patient population when they extend far beyond ED walls?
An Example Case
In June 2025, an ED at a large, urban, multi-site academic health system organized and facilitated a system-wide panel of about 20 experts in the care of patients with OUD. Experts included emergency clinicians, psychiatrists, pain specialists, community-based primary care physicians, informaticists, population health specialists, and more. These experts came from multiple hospital and outpatient sites, many without existing working relationships or prior interpersonal connections. Over four hours, this expert panel outlined the care journey for patients with OUD across the health system, with attention to identifying care gaps, and subsequently brainstorming solutions.
An executive summary that included a qualitative situation assessment, in addition to an organized list of gaps, potential solutions, and outstanding questions, identified poor standardization of care and frequent loss to follow up as major issues. Potential solutions ranged from easy-to-implement quick wins, such as scaling existing interventions to new care sites within the health system, to bigger picture system-level changes, with examples included in Table 1.
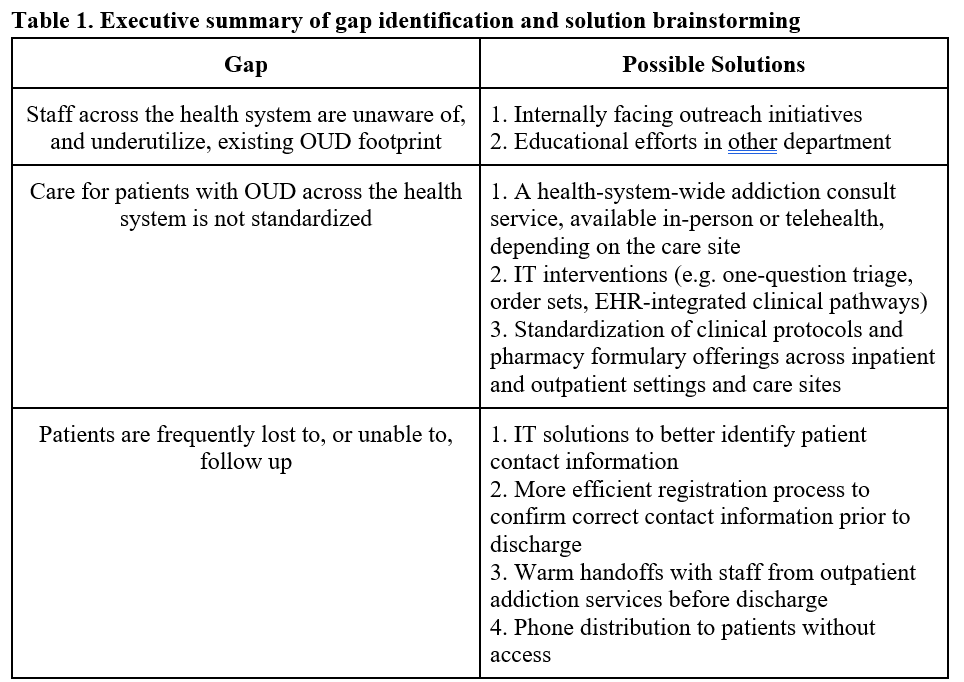
Click to enlarge.
In the months since completion, this summary has been socialized with health system leadership. It now factors into ongoing decision making about resource allocation and intervention prioritization. In returning to their respective functions across the health system, panel experts are using this summary as a tool to inform their future areas of investigation and intervention. Specific projects initiated following this panel include: (1) creating a health system-wide, EHR-integrated clinical pathway guiding withdrawal management to standardize care across different care sites, (2) improving care coordination at transition points, including transfers to inpatient detoxification and discharge referrals to outpatient resources, (3) streamlining EHR-integrated best practice advisories and order sets to optimize treatment prescribing and referral, and (4) building a case for increased access to addiction-trained subspecialists. Additional projects addressing gaps identified through this panel are expected in the coming months.
Pages: 1 2 3 | Single Page




No Responses to “Emergency Medicine as Leaders in Care Provision for Patients with Opioid Use Disorder”