
We believe that naltrexone is the most effective MAUD, the easiest to initiate in the emergency department, and should be used for patients who are interested in reducing cravings and cutting down on their alcohol intake. The outline below discusses our thought process of how to effectively implement a screening and treatment program for alcohol use disorder in your ED.
Explore This Issue
ACEP Now: February 2026 (Digital)1) Develop a universal screening program for Alcohol Use Disorder
- Work with administration, ED staff, and nursing to develop a universal screening program in your ED.
- Use the screening tools and resources that are available and work most effectively in your health care facility.
2) Implement a screening protocol in your ED
-
- Use STAD or SASQ for all patients in intake.
- Use the AUDIT-C for those who have screened positive.
3) Motivational Interviewing
- For patients who had a positive screening or endorsed an interest in reducing their alcohol use, take the time to discuss their alcohol use, and better understand their thoughts about its impact on their health.
4) Gauge Interest in MAUD
- Ask about the patient’s interest in starting potential treatment options such as naltrexone or acamprosate.
5) Discuss Naltrexone
- Offer naltrexone, as it is the best option for treating AUD in most circumstances.
- Ask about the patient’s opioid use history, if the patient has a history of opioid use or current opioid use, then discuss acamprosate.
6) Start MAUD
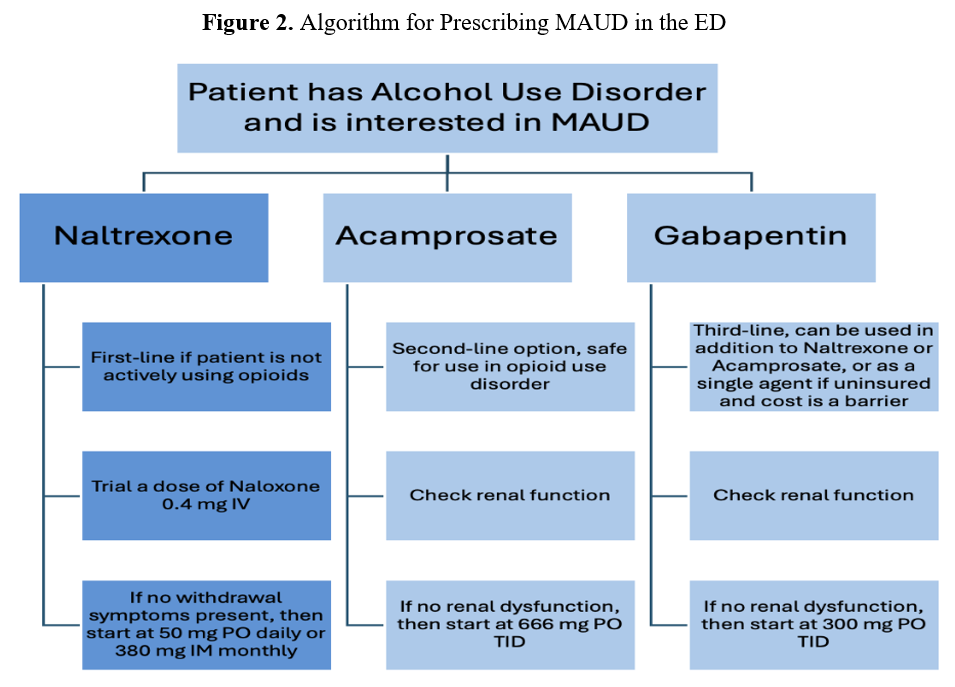
Click to enlarge.
- Naloxone Challenge: Administer a 0.4 mg IV naloxone dose. It will help to determine if naltrexone would precipitate withdrawal.
- If precipitated withdrawal occurs, then manage with buprenorphine or adjunctive therapies (clonidine, Zofran, loperamide, etc.).
- If no precipitated withdrawal occurs, proceed with treatment.
- Oral: Start with 50 mg PO naltrexone.
- Injectable: Start with 380 mg IM naltrexone.
- If any contraindications to Naltrexone, then initiate acamprosate 666 mg PO TID.
7) Discharge Planning
- If PO naltrexone is administered, then discharge the patient with a 14- to 30-day prescription (50 mg daily).
- If IM naltrexone is given, then arrange follow-up for the patient in one month for the following dose.
- Ensure that all patients have follow-up with a primary care physician (PCP) and addiction medicine physician.
Emergency physicians trailblazed the management of opioid use disorder and the initiation of medications such as buprenorphine. The management of AUD should be no different. The ED is often the only contact between the community and the health care system, and AUD is a condition that impacts numerous individuals seen daily. Each opportunity that we have with a patient with AUD is an opportunity to intervene, discuss resources, and potentially start treatment.




No Responses to “Alcohol Use Disorder: Screening Tools and Medications in the ED”