
Alcohol use disorder (AUD) is often seen as a primary problem in the emergency department (ED) but can also be an impactful underlying condition for many other presentations. Each time we see a patient with a significant alcohol use history, we need to ask, “Could this be an opportunity to intervene in their alcohol use? What can we offer them in the ED today to manage their AUD? How can we break the cycle of problematic drinking?”
Explore This Issue
ACEP Now: February 2026 (Digital)AUD is specifically defined as a “problematic pattern of alcohol use leading to clinically significant impairment or distress,” characterized by a relapsing and remitting pattern of use, that impacts roughly 29 million individuals throughout the nation.1,2 Based on the DSM-5 criteria, it can be classified as mild, moderate, or severe based on the presence of various symptoms.2
Emergency departments are often the only interaction that many patients have with the health care system. However, we regularly fail to address the consequences of alcohol consumption. AUD is frequently not the primary complaint patients have when seeking treatment at an ED, and it is often not apparent that patients are dealing with this condition, but it may be the underlying cause. This complexity further hampers the accurate identification of patients with this condition who would benefit from appropriate treatment. From 2021 to 2023, alcohol-related ED visits made up about nine million cases, double the number of opioid-related visits.3 This represents a 50 percent rise in alcohol-related visits since the early 2000s.4
But there is precedent that can guide our approach to this problem. Emergency physicians have led the charge in confronting opioid use disorder and reducing overdose deaths through initiating medications like buprenorphine. Emergency physicians can quickly identify and treat alcohol withdrawal syndrome and many of the immediate life-threatening issues associated with alcohol use and can improve upon treating the underlying use disorder. Medications for Alcohol Use Disorder (MAUD) are rarely prescribed in the ED, with data demonstrating that less than 1 percent of AUD patients are initiated on treatment annually.5 Every ED encounter is an opportunity to intervene, screen, educate, and potentially start effective treatment options that can prevent adverse outcomes.
Screening for Alcohol Use Disorder
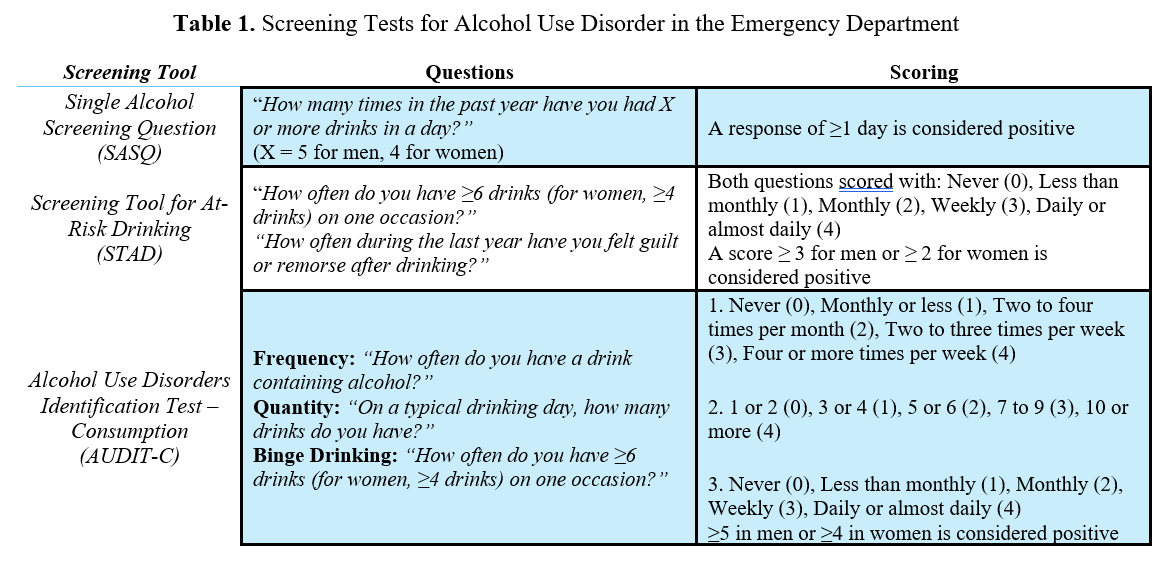
All tables courtesy Dr. Imperato. Click to enlarge.
One of the main challenges in treating AUD is properly identifying patients with AUD. Currently, roughly 8 percent of patients who present to the ED are screened.6,7 Multiple tools exist to screen for AUD. Some of the more thorough tools include the DSM-5, the Alcohol Use Disorders Identification Test (AUDIT), the Michigan Alcoholism Screening Test (MAST), and the short MAST (sMAST). While these tools are time-consuming and less likely to be effectively utilized on a wide scale in EDs, the following tools are concise and can be rapidly used to screen for AUD.




No Responses to “Alcohol Use Disorder: Screening Tools and Medications in the ED”