Flexible Geography
Since your peri-pandemic emergency department will need to be a different emergency department on any given day, with volume and acuity swings that are extreme, you need to think about how to accommodate the variation within the physical space.
Explore This Issue
ACEP Now: Vol 40 – No 10 – October 2021- Flex Unit: A combined unit that can flex with the acuity distribution is an idea whose time has come. Here are a few examples of flex units:
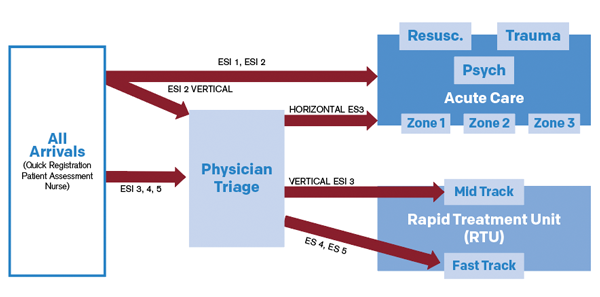
- Perhaps the most common example is the rapid treatment unit idea. The Tennity Emergency Department at Eisenhower Health in Rancho Mirage, California, designed a space that combines the fast track and the mid track (see Figure 1). Middle- and lower-acuity volumes showed the most variation in the peri-pandemic months, so this space was ideal for them, and patients were treated predominantly in recliners in this area. APPs saw the low-acuity patients and helped with some easier mid-track patients, who were predominantly managed by physicians. (See the February 2021 issue of ACEP Now for more on Tennity’s flexible ED design.)
- Conversely, an ED patient care area can be flexed into a boarding unit. At the Christiana Care emergency department in Wilmington, Delaware, a dual-purpose 11-bed “core” was identified as a flex zone. This area could be a lower-acuity zone, boarding unit, or hybrid unit based on the conditions of the day. An APP managed both groups of patients, and staffing was flexed accordingly. If this pod was used primarily for boarding and no new patients could be processed there, physician hours were saved by sending the clinician home.
- At Hasbro Children’s Hospital in Providence, Rhode Island, variation in both orthopedic surges and behavioral health surges were noted. Orthopedic cases peak in the summer, while behavioral health cases peak when school starts through the winter. The hospital has a zone that functions alternatively as an orthopedic suite or behavioral health holding suite based on the patient numbers each day. (See the March 2018 issue of ACEP Now for more on Hasbro Children’s Hospital’s efforts to improve metrics.)
- Flex Beds: A variation of the flexible geography concept is to identify flex beds or treatment spaces with proximity to a zone. This patient-centered approach was used at Washington Hospital Healthcare System in Fremont, California, in its new emergency department. It also helps when two clinicians have vastly different productivity and efficiency levels. This model allows each to work at their own pace by giving the clinicians more rooms to see patients when they can and fewer rooms when they can’t see the next new patient quickly. Figure 2 depicts two zones and a group of shared beds that can be part of either zone. (See the March 2019 issue of ACEP Now for more on Washington Hospital’s approach to moving to a larger ED space.)

Figure 2: With the flex-bed concept, two zones share
a group of flexible beds that can be part of either zone.
Flexible Shifts
Volume swings of 40 percent will always need adjustments in staffing. Helen DeVos Children’s Hospital in Grand Rapids, Michigan, created a model of flexibility in scheduling. Its shifts match the patient arrivals, not physician or nursing preference. The physicians have flexible shifts called “at-risk shifts.” These flex shifts may be four, eight, or 12 hours, depending upon departmental conditions. A real-time huddle of physician and nurse leaders is held to decide the strategy for opening and closing of zones in real time. Predetermined rules decide if and when the clinician goes home. They have well-articulated processes for most contingencies. (See the July 2019 issue of ACEP Now for more on Helen DeVos’s data-driven ED flow.)
Pages: 1 2 3 | Single Page




No Responses to “Strategies To Help Your ED Adapt to Variable Volumes and Patient Needs”