Don’t Wait to Make the Call
Early ENT consultation is crucial, particularly in rural settings with limited access to specialized care. Secondary post-tonsillectomy hemorrhages often require surgical intervention. The literature suggests that approximately 85 percent of these cases require procedural source control in the operating room, highlighting the importance of expediting transport arrangements.5
Explore This Issue
ACEP Now: Jan 01Temporizing Measures
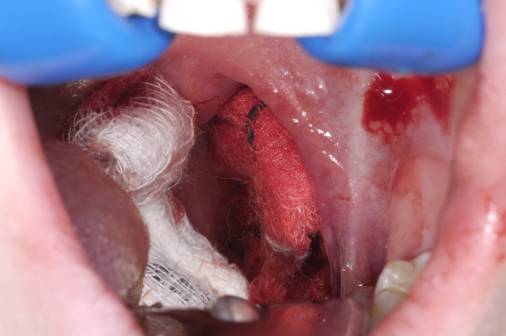
Temporizing measures are vital while awaiting transport, as they help to stabilize the patient and prevent further deterioration. First, lidocaine spray can be used for local analgesia, increasing patient tolerance.6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention.7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression. For topical application of medications, a hack that I’ve found useful is utilizing a see-through plastic vaginal speculum with a built-in light; it gives great exposure, great lighting, and great access to the point of maximal bleeding.
TXA can be administered in three ways: nebulized, topical, or intravenous. Each method has a role in managing secondary post-tonsillectomy bleeds, although evidence is limited to case studies and small observational trials with variable results.7,8 Nebulized TXA can be thought of as a “set it and forget it” intervention. Put it on early while you’re managing other tasks; it requires minimal involvement and frees you up for other essential steps. Gauze soaked in TXA applied to the tonsillar fossa provides localized bleeding control. IV TXA one to two grams in adults, or 15 mg/kg in children over 10 minutes, offers another layer of control, particularly when topical TXA alone does not suffice. The evidence may be sparse, but TXA in any form is generally safe in patients without obvious thrombotic contraindications.
Lastly, an antiemetic such as IV ondansetron is recommended to prevent vomiting, which can exacerbate bleeding or dislodge forming clots. Controlling nausea may also reduce the risk for gag reflex activation during oropharyngeal manipulation, further minimizing trauma.
Airway Management
If bleeding worsens and the patient shows signs of aspiration or respiratory distress, such as desaturation or altered mental status, securing the airway may become necessary. Be prepared for all but the most trivial bleeds with a double suction setup and video rapid sequence intubation (RSI) as you might in the setting of massive hemoptysis.9 Have two suction devices ready—ideally meconium aspirators or DuCanto catheters, which allow for superior fluid clearance from the oropharynx compared with Yankauer catheters.10 Careful, smooth RSI with video laryngoscopy is the preferred airway strategy, as it is likely to give you the best view while minimizing the need for multiple attempts, which may increase bleeding from localized trauma.
Pages: 1 2 3 4 | Single Page




4 Responses to “Post-Tonsillectomy Hemorrhage: A Three-Pronged Approach”
January 15, 2025
Creed MamikunianAs an ENT who has practiced for 35 years, I usually managed these patients in the ER awake. Spray topical lidocaine on the side bleeding. Then inject about 2-3 cc 1% lidocaine with epi at the site of bleeding. You need a strong headlight from the OR and a suction bovie machine also from the OR. Have your ENT teach you how to use these various instruments, they are your friend. Calmly talk the patient through what you’re doing and then cauterize the bleeding vessel. It’s usually at the plica triangularis (the bottom of the tonsillar fossa. Use two tongue blades to push the tongue down to find the bleeder. Give it a few good buzzes with the suction bovie and you’re done.
Everything else is just delaying the treatment. One last thing, if it’s a young patient, this won’t work. Teenagers at a minimum. Otherwise, you’d better hope your ENT is close by.
January 19, 2025
Paul MMany of us live in a world where there is no ENT…either on call or close by. Top 5 bad cases at 0300….tonsillar bleed in pediatric patient.
February 20, 2025
Dr James C MartinHaving practiced ENT for 35+ yrs, I’ve seen my share of post-tonsil bleeds, usually 5-10 days postop, but have seen them as late as several weeks. I don’t hesitate to take these patients to the OR, not only for excellent visualization, but there’s nothing worse than stopping the bleeding in the ER, only to be called back 2-3 hrs later because the patient rebled, usually secondary to N/V at home despite anti nausea meds.
Usually cautery or coblation solves the problem, and I then inject 1-2cc of 1/4% marcaine with 1/200K epinephrine for pain control, along with hemostatic effect.
Postop tonsil bleeds can be severe and cause you to age faster, and loose sleep!
July 26, 2025
Dee EmersThis sentence here “Calmly talk the patient through what you’re doing and then cauterize the bleeding vessel.” Was so nice to read. My son went through this and it was so scary for him and myself because no one explained anything and the blood was so scary for us to see. Possibly the people in ED didn’t know what was going on until the ENT arrived. Not sure but it was traumatizing for my 7 year old.