Emergency physicians have been tasked not only with providing safe and accurate care but also with stewardship of society’s scarce resources. Among other things, this means outpatient management of some disease entities traditionally managed in an inpatient setting.
Explore This Issue
ACEP Now: Vol 35 – No 08 – August 2016Deep vein thrombosis (DVT) is a relatively common condition, having lifetime prevalence of up to 5 percent, and is commonly first diagnosed in the emergency department.1,2 Massive proximal DVT can lead to phlegmasia alba, which is itself limb-threatening. Pulmonary embolism is a frequent complication, and in patients with patent foramen ovale, paradoxic/systemic thromboembolic complications such as stroke can develop. Late morbidity of venous thromboembolism (VTE) such as postphlebitic syndrome characterized by extremity edema and pain, stasis dermatitis, and, in severe cases, ulcer formation, as well as pulmonary hypertension, is well-described. Timely therapy reduces the rate of these complications.
Systemic anticoagulation for DVT may include therapeutic dosages of unfractionated heparin, low-molecular-weight heparin (LMWH), rivaroxaban, or fondaparinux. Alternatives such as vena cava filters and mechanical clot removal in patients with contraindications to anticoagulation exist, but they are outside the practice of emergency medicine. Since development of LMWH in the late-20th century, the option for discharge of select patients with DVT from the emergency department became viable. This has the potential to improve quality of life, increase patient convenience, and reduce health care expenditures.1,3–5 Outpatient management of DVT was slow to catch on. One report of patients diagnosed with DVT treated from 2003 to 2007 noted that only 28 percent of patients were treated as outpatients.6
After the diagnosis is established, it should be decided if the patient is appropriate for outpatient management. Those with iliofemoral clot, unstable clot visualized on ultrasound, severe comorbid conditions, or unstable social situations make poor candidates for discharge from the emergency department. There is a paucity of data on outpatient management of upper-extremity DVT. Special attention should be paid to the patient’s risk of bleeding once anticoagulated. In addition to the physician’s judgment, there are tools such as the Registry of Patients with Venous Thromboembolism (RIETE) score (available at www.mdcalc.com/riete-score-risk-hemorrhage-pulmonary-embolism-treatment) for assistance in determining suitability for outpatient management. Patients judged to be a higher risk should be given an easily reversible agent and monitored in the hospital initially.
Since development of LMWH in the late-20th century, the option for discharge of select patients with DVT from the emergency department became viable. This has the potential to improve quality of life, increase patient convenience, and reduce health care expenditures.
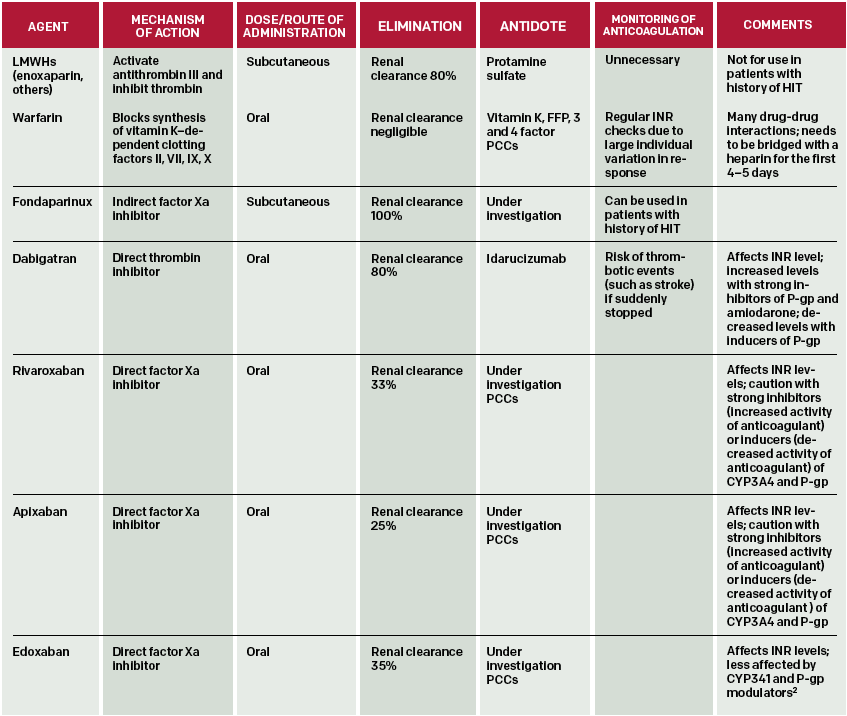
(click for larger image)
Table 1: Options for Outpatient Anticoagulation in Patients with DVT.1,9
Pages: 1 2 3 4 | Single Page




4 Responses to “Options, Approaches to Outpatient Treatment of Deep Vein Thrombosis for Emergency Physicians”
August 24, 2016
Sunjeev Konduru, MS, PharmD, BCPSThe dosing of apixaban in this article does not match the FDA prescribing information, which states give 10mg twice a day for 7 days, followed by 5mg twice a day. This dose of Eliquis was studied in the AMPLIFY trial for 6 months versus lovenox and warfarin in patients with symptomatic PE or proximal DVT.
Edoxaban also required initial parenteral anticoagulation for 5 to 10 days, similar to dabigatran.
Thank you.
August 28, 2016
jakeYou correctly point out dabigatran as a direct thrombin inhibitor in the text of the article, however, in the table it is incorrectly listed as a Xa inhibitor.
August 30, 2016
Dawn Antoline-WangThank you, the table has been updated to reflect this correction.
August 29, 2016
Soumya Ganapathy MDGreat article. When treating DVTs and PEs as an outpatient, patient education is paramount. Patient and their families can often feel overwhelmed. ACEP has a program called knowbloodclots.com, it is a great resource for patient education on DVTs and PEs. They have nice videos like what to expect with DVT and PE treatment as well as warning videos on the risk of bleeding. They also have a free texting program that sends reminders and educational links to patients.