
Sonoanatomy
Place the high-frequency linear transducer above the upper border of the mid-to-lateral clavicle in a coronal oblique plane (parallel to the clavicle and aiming the beam into the thorax) (Figure 1B). Move the transducer medially to find the anechoic, round, and pulsatile subclavian artery (can be confirmed by color Doppler). The brachial plexus often appears superior and lateral to the artery, and often looks like a “cluster of grapes.” Note the first rib, a hyperechoic line with distal shadowing just under the brachial plexus. This should be contrasted to the normal lung sliding in the far field (Figure 2). In many patients, the first rib may not be clearly seen and the clinician will have to rotate the tail of the transducer in a counterclockwise manner to bring this sonographic landmark into view (Figure 3).
Explore This Issue
ACEP Now: Vol 42 – No 04 – April 2023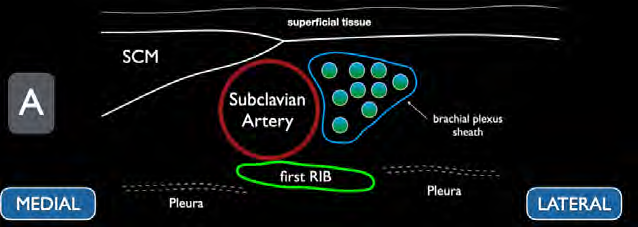
FIGURE 2A: Schematic representation of the supraclavicular brachial plexus. (Click to enlarge.)
An alternative technique, should you have difficulty finding the brachial plexus, is to start in the neck by identifying the carotid artery and internal jugular vein about the level of the cricoid cartilage.8 Slide the probe inferiorly toward the clavicle, reducing the angle between the probe and the skin as the probe is moved. In addition to using the subclavian vessels as a landmark, also be sure to identify any other vascular structures in the area of interest. After locating the brachial plexus and the projected needle path, we recommend use of color Doppler to prevent inadvertent vascular puncture.10
FIGURE 2B: Ultrasound image of the supraclavicular brachial plexus. (Click to enlarge)
Performing the Block
Once the optimal transducer position and needle path is identified, place a small skin wheal of local anesthetic just lateral to the transducer to anesthetize the overlying skin. After properly disinfecting the skin, enter through the skin wheal for a lateral to medial in-plane approach with the nerve block needle. Ensure continuous needle visualization and advance the needle tip until it touches the first rib. The goal is to find the area between the first rib and nerve bundle to inject anesthetic. Once you have clear needle-tip visualization within this space and have gently aspirated to ensure the needle tip is not intravascular, we recommend gently injecting a small amount of normal saline to ensure proper spread of anechoic fluid (hydrodissection).
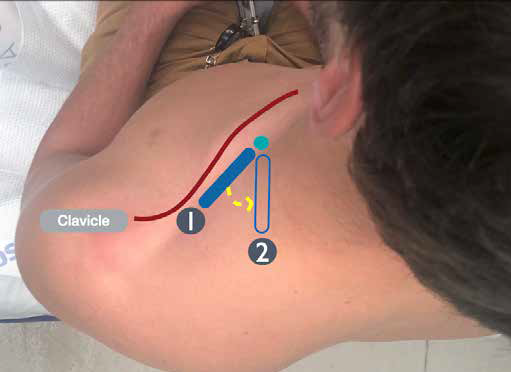
FIGURE 3: By rotating the ultrasound probe in a counterclockwise manner, the first rib can often be seen more clearly in cross-section on ultrasound. (Click to enlarge.)
Pages: 1 2 3 4 5 | Single Page




No Responses to “How To: The Ultrasound-Guided Supraclavicular Brachial Plexus Block”