Explore This Issue
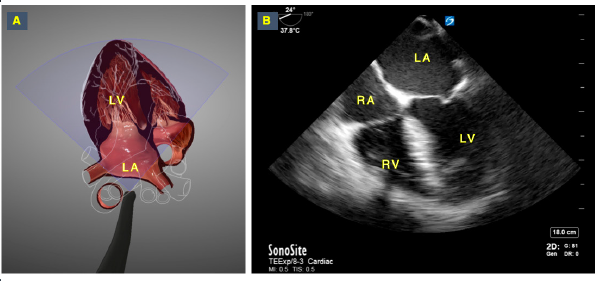
ACEP Now: Vol 39 – No 07 – July 2020Figure 5: Retrocardiac “point of view” of the TEE probe. Image A shows the TEE probe’s point of view, which provides sonographers with an ideal perspective to understand the spatial orientation and anatomical relationships needed to develop and interpret TEE views. Image B shows the corresponding mid-esophageal 4 chamber view in TEE, with the left atrium in the near field.
3-D graphics reproduced with permission by HeartWorks Intelligent Ultrasound
How to Perform Resuscitative TEE
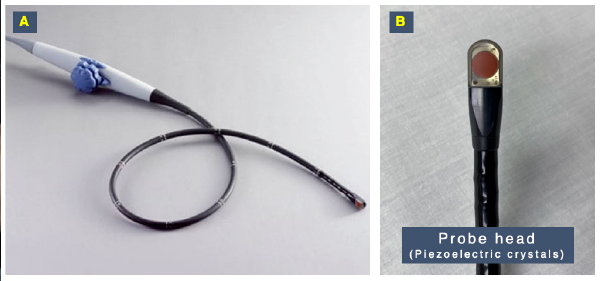
TEE Probe Knobology: In place of the normal hand movements used when performing TTE (eg, fanning, sliding, rotating, etc.), the TEE probe uses mechanical digital components to produce the desired images. The endoscopic shaft may be advanced, withdrawn, and turned to locate the heart. The lockable wheels on the handle then help produce the various movements similar to tilting, fanning, and rocking the probe by anteflexing and retroflexing the transducer (see Figures 1 and 2).
In addition to these mechanical controls, digital components allow for rotation of the imaging plane itself (the ultrasound beam) in a 180° plane. This is referred to as the omniplane, and it’s displayed by a half circle with a range of 0–180° located at one of the top corners of the screen. The utilization of the omniplane allows for further characterization and detailed views of the heart and surrounding structures. This movement is similar to looking at structures in the long and short axis when utilizing a TEE probe (see Figure 3).
Probe Insertion: Resuscitative TEE is generally performed only in intubated patients. The placement of the TEE probe is performed similarly to the placement of an orogastric tube. The flexion wheels are first placed in the unlocked position to allow for free movement of the probe tip. With the transducer facing anteriorly, the probe is advanced into the mouth and pharynx under direct vision and manual guidance to maintain midline position.
The most common anatomical sites causing obstruction of the TEE probe during insertion in an intubated patient are the arytenoid cartilage and the pyriform fossa. Therefore, to access the esophagus and avoid pharyngeal injuries, it is critical to keep the probe at the midline while advancing it. This can be performed by either digitally guiding the probe or under direct visualization with a video laryngoscope.
To aid in the passage of the probe tip past the upper esophageal sphincter, the mandible may be pulled forward gently and the patient’s neck partially flexed. Be careful not to dislodge the endotracheal tube (see Figure 4).
Acquiring and Interpreting TEE Images: Understanding the anatomical position of the heart is fundamental to the practice of echocardiography and particularly for TEE. A new mental representation of the cardiac anatomy is required to comprehend how images are generated from the esophageal position when performing TEE. This is the view most anatomy textbooks and echocardiography learning resources use to display the heart, and it is the view that makes the most sense to understand how TTE views are generated.
On the other hand, to interpret TEE views, a different anatomical perspective must be understood. The TEE probe head is located in the esophagus and obtains images from a retrocardiac perspective. This inverted imaging position is often difficult for even seasoned TTE sonographers, but it is the starting point in understanding TEE imaging. Simply put, this new perspective is the view of the heart and great vessels as seen by the TEE probe when the image is generated from the esophageal position. This retrocardiac perspective facilitates the understanding of how the different mechanical and digital movements in TEE generate the views obtained while using this modality (see Figure 5).




No Responses to “How to Perform Resuscitative Transesophageal Echocardiography in the Emergency Department”