Evaluating “Good” Against Alternatives
This brings us to the elephant in the room: the lack of any meaningful comparison arm. While those designing this study seemed to feel that a control arm was unwarranted or unethical, there is an obvious and clear alternative available, prothrombin complex concentrate (PCC). The most typically used four-factor PCCs include factors II, VII, IX, and X, along with proteins C and S. While PCCs are indicated primarily for the urgent reversal of vitamin K antagonists, they are also recommended, by guidelines, for the treatment of anti–factor Xa–related hemorrhage.3 Should the specific but finite nature of andexanet make it the preferred approach, or do we need a prospective comparison with PCCs to determine its utility?
Explore This Issue
ACEP Now: Vol 38 – No 04 – April 2019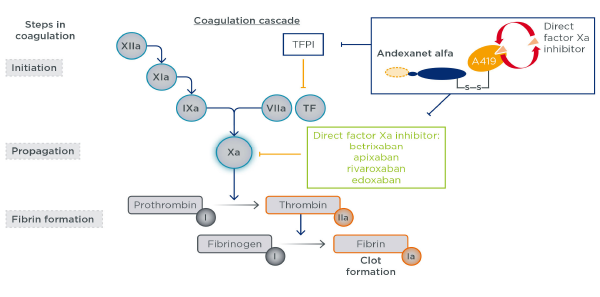
Figure 1: Andexanet alfa mechanism of action
Andexanet alfa is a recombinant modified FXa protein with no enzymatic activity, designed to bind and sequester FXa inhibitors and thus reverse anticoagulation.
EMJ Cardiol. 2018;6(1):47-51. CC-BY NC 4.0
The answer is clearly the latter, as plans for such a study are already underway (ClinicalTrials.gov number: NCT03661528). While cost and value assessments are difficult when faced with life-threatening complications, it is recognized by all parties that we need additional data to determine when, or if, andexanet should be used. The costs of PCCs are already imposing, with a typical dose priced around $5,000. Andexanet takes this to another level, with the cost up to $50,000 for the high-dose protocol.4 While these costs may be comparable to other lifesaving therapies and interventions, it is an impressive ask to consider this therapy without data demonstrating its clinical superiority over an alternative a tenth the cost.
It should also be noted that nearly 30 percent of those in this trial treated with andexanet were ultimately excluded from the efficacy analysis, owing primarily to anti–factor Xa levels lower than the prespecified threshold requiring treatment. The lack of reliable initial tests to verify the presence of deranged coagulation is not unique to the factor Xa inhibitors, but it is decidedly unpalatable to consider the extent to which patients may be unnecessarily treated with this expensive therapy.
Finally, although the primary concern is comparative efficacy to care with PCCs, there is also concern regarding adverse effects. Andexanet does not only bind anti–factor Xa but also tissue factor pathway inhibitor (TFPI). Without rehashing everyone’s favorite coagulation cascade from medical school, the “inhibitor” portion of TFPI prevents unwanted coagulation. Animal studies conducted by the manufacturer suggest andexanet binding TFPI should not result in excess adverse effects, specifically in those patients who might be inadvertently treated. However, these conclusions cannot be confirmed or refuted by those data.5 Overall, 10 percent of those treated with andexanet developed a thrombotic event within 30 days, half of which were arterial (eg, stroke or myocardial infarction). While PCCs are not free of associated thrombotic harms, this safety comparison is also critical to the follow-up clinical trial.
In the meantime, until clearer data arrive, andexanet is best left on the sidelines. Furthermore, by the time the follow-up trial is conducted, consideration of andexanet may be moot, as its competitor, ciraparantag, is on the horizon.6 Preclinical data suggest this molecule may be a universal antidote to all heparins and oral anticoagulants, but as we’ve seen with andexanet, it is no small feat to live up to the hype.
Pages: 1 2 3 | Single Page


No Responses to “Factor Xa Inhibitor Reversal Agent Is Not Ready for Prime Time”