Future Uses and Suggestions
Care needs to be taken as to the number of layers of fiberglass used to create the skull. We found that too many or too few layers created less than realistic conditions for drilling. Three layers of fiberglass seemed to provide adequate thickness.
Explore This Issue
ACEP Now: Vol 41 – No 10 – October 2022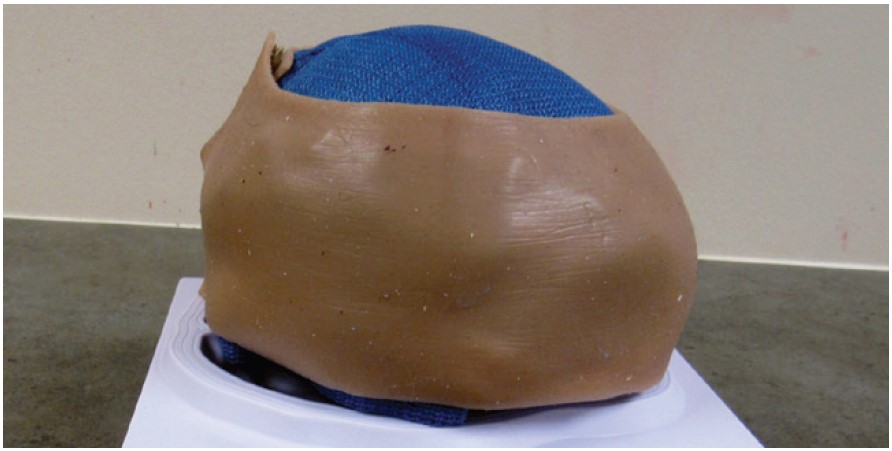
FIGURE D: Repairable simulated neck skin. Obtained from Strategic Operations, Inc., San Diego, CA—$52.
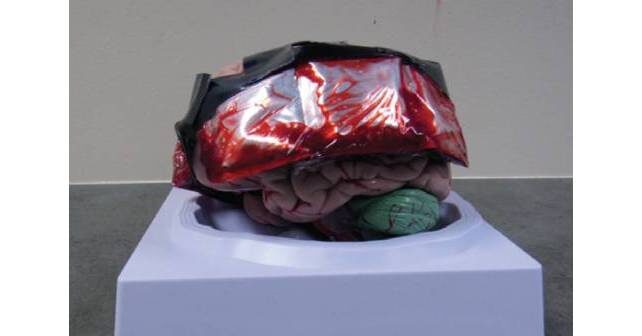
There are a few limitations with our model, as we originally developed it. Therefore, we suggest that this model can be modified and improved upon to provide a more realistic task trainer for the burr hole procedure. These modifications result in an even simpler construction of the model. Subsequently, we have found that using a 2-inch by 2-inch, 4-mm, resealable plastic packet filled with ten to 15 mL of artificial blood (Figure F) resulted in more predictable “blood” flow after drilling and avoided leakage as was sometimes seen from the ice-pack segments. We have also found that using a commercially available, stretchable “skull cap” to cover the fiberglass material serves as a good base for a silicone skin pad which is glued to the skullcap. The silicone skin pad can be made relatively inexpensively, or purchased, and used as an alternative to the commercial neck skin that was used initially (Figure G).

FIGURE E: Medical students simulating the burr hole procedure at Rocky Vista University College of Osteopathic Medicine, MCI training.
When implementing the use of a trephine drill in actual clinical practice, there are other options available, as the Galt trephine seems less utilized in current patient care settings. Cranial access kits can be purchased utilizing an internet search. These kits typically consist of a rotary, hand powered drill. They also provide different drill bit sizes, as well as a stopper to control depth of drilling. Cranial access kits may be used by neurosurgeons to place ventriculostomies. At the time of this writing, these kits cost approximately $1,100. Our model should be a good simulation platform for use with cranial access kits, as well as the Galt trephine drill.
Conclusion

FIGURE F: Transparent plastic bag, two inch by two inch (resealable) from Amazon.com—$7.99.
Emergency trephination is a low-frequency, high-risk procedure. To our knowledge, there are no inexpensive portable trainers available for this procedure. Our model attempts to address this gap. We believe that with future refinements, the model may serve an important role in the training of emergency physicians and other non-neurosurgeons in the performance of this skill.
Pages: 1 2 3 4 | Single Page


No Responses to “Emergency Department Trephination (Burr Hole) for Epidural Hematoma”