Explore This Issue
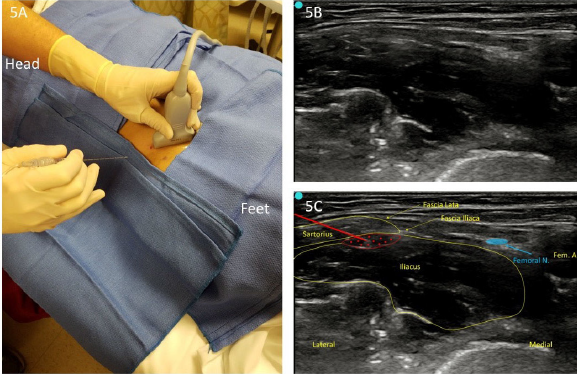
ACEP Now: Vol 37 – No 01 – January 2018Figure 5. A: Suprainguinal approach (lateral to medial). B: Unlabeled infiltration view. C: Labeled infiltration view.
Summary
A multimodal pain management approach that incorporates USGFICB for patients with acute femoral neck fractures has been demonstrated to reduce the reliance on opioids.16 Specifically in the elderly patient, this bedside intervention can reduce unwanted side effects commonly seen with opioids while offering significant pain control. USGFICB may be an ideal option for sonographers who are less comfortable performing USGFNB.
Dr. LaJeunesse is a captain in the U.S. Army Medical Corps and a second year EM resident at Madigan Army Medical Center (MAMC) in Tacoma, Washington. Mr. Cronin is a major in the U.S. Army Medical Specialist Corps and program director and assistant professor of the U.S. Army-Baylor University emergency medicine PA residency at MAMC. Dr. Takahashi is a captain in the U.S. Army Medical Corps, a family medicine physician, and an emergency ultrasound fellow at MAMC. Mr. Knudsen is a captain in the U.S. Army Medical Specialist Corps and an emergency medicine resident and doctoral candidate at MAMC. Dr. Nagdev is director of emergency ultrasound at Highland Hospital, Alameda Health System, in Oakland, California.
References
- Hip fractures among older adults. Centers for Disease Control and Prevention website. Accessed Dec. 14, 2017.
- Mutty CE, Jensen EJ, Manka MA Jr, et al. Femoral nerve block for diaphyseal and distal femoral fractures in the emergency department. J Bone Joint Surg Am. 2008;90(Suppl 2 Pt 2):218-226.
- Mouzopoulos G, Vasiliadis G, Lasanianos N, et al. Fascia iliaca block prophylaxis for hip fracture patients at risk for delirium: a randomized placebo-controlled study. J Orthop Traumatol. 2009;10(3):127-133.
- Foss NB, Kristensen BB, Bundgaard M, et al. Fascia iliaca compartment blockade for acute pain control in hip fracture patients: a randomized, placebo-controlled trial. Anesthesiology. 2007;106(4):773-778.
- Odor Pm, Chis Ster I, Wilkinson I, et al. Effect of admission fascia iliaca compartment blocks on post-operative abbreviated mental test scores in elderly fractured neck of femur patients: a retrospective cohort study. BMC Anesthesiol. 2017;17(1):2.
- Grabinsky A, Sharar SR. Regional anesthesia for acute traumatic injuries in the emergency room. Expert Rev Neurother. 2009;9(11):1677-1690.
- Reavley P, Montgomery AA, Smith JE, et al. Randomised trial of the fascia iliaca block versus the ‘3-in-1’ block for femoral neck fractures in the emergency department. Emerg Med J. 2015;32(9);685-689.
- Hogh A, Dremstrup L, Jensen SS, et al. Fascia iliaca compartment block performed by junior registrars as a supplement to pre-operative analgesia for patients with hip fracture. Strategies Trauma Limb Reconstr. 2008;3(2):65-70.
- Dochez E, van Geffen GJ, Bruhn J, et al. Prehospital administered fascia iliaca compartment block by emergency medical service nurses, a feasibility study. Scand J Trauma Resusc Emerg Med. 2014;22:38.
- McRae PJ, Bendall JC, Madigan V, et al. Paramedic-performed fascia iliaca compartment block for femoral fractures: a controlled trial. Journal Emerg Med. 2015;48(5):581-589.
- Swenson JD, Davis JJ, Stream JO, et al. Local anesthetic injection deep to the fascia iliaca at the level of the inguinal ligament: the pattern of distribution and effects on the obturator nerve. J Clin Anesth. 2015;27:652-657,
- Kardash K, Hickey D, Tessler MJ, et al. Obturator versus femoral nerve block for analgesia after total knee arthroplasty. Anesth Analg. 2007;105(3):853-858.
- Gadsden J. Local anesthetics: clinical pharmacology and rational selection. The New York School of Regional Anesthesia website. Accessed Dec. 15, 2017.
- Wolfe JW, Butterworth JF. Local anesthetic systemic toxicity: update on mechanisms and treatment. Curr Opin Anaesthesiol. 2011;24:561-566.
- Hebbard P, Ivanusic J, Sha S. Ultrasound-guided supra-inguinal fascia iliaca block: a cadaveric evaluation of a novel approach. Anaesthesia. 2011;66(4):300-305.
- Groot L, Dijksman LM, Simons MP, et al. Single fascia iliaca compartment block is safe and effective for emergency pain relief in hip-fracture patients. West J Emerg Med. 2015;16(7):1188-1193.
Pages: 1 2 3 4 | Single Page




5 Responses to “Control Hip Fracture Pain Without Opioids Using Ultrasound-Guided Fascia Iliaca Compartment Block”
January 27, 2018
Ron BraceThe diagram, first color coded one showing locations of Fem nerve vein and artery is seriously mislabeled and a correction need be done; Femoral Vein is in wrong place, as is the Femoral artery – and the fem artery is mislabeled
I am sure by now a thousand people have written about it!
https://www.acepnow.com/wp-content/uploads/2018/01/ACEP_0118_pg20a.png
January 28, 2018
Robert A.Great article. I think Figure 1 is mislabeled: Femoral artery is mislabeled as “Fem V.” and Femoral vein mislabeled as “Fem N. (red)”.
February 5, 2018
HosamIn illustration, I think that order of structures are not proper.it is vien artery nerve from medial to lateral
February 5, 2018
MikeHi, picture 1 seems to have some errors. There are two structures markes Fem N, one of them in red which is likely supposed to be the Fem Artery. If that structure is supposed to the fem artery it is incorrectly positioned medial to the femoral vein when it should be lateral
February 5, 2018
Dawn Antoline-WangThank you to everyone who pointed out the error in Figure 1. The image has been corrected.