A 45-year-old female presented to the emergency department approximately three hours after a suspected intentional multidrug overdose, which included extended-release bupropion and amitriptyline among several other medications. On arrival, the patient exhibited tonic-clonic seizures and required emergent endotracheal intubation. Her vital signs were notable for profound hypotension (BP 51/35 mmHg) and relative bradycardia (HR 68 bpm).
Explore This Issue
ACEP Now: November 2025An initial ECG revealed a widened QRS (136 ms) and prolonged QTc (521 ms). Vasopressor support with norepinephrine was initiated, and sodium bicarbonate therapy was started and titrated to a serum pH of 7.50-7.55, resulting in QRS narrowing. This initial management stabilized her hemodynamics, but despite aggressive supportive care, her neurologic exam showed absent brainstem reflexes. These findings raised concern for irreversible anoxic brain injury versus pharmacologic brain death due to drug toxicity.
Diagnosis and Management
This case represents a rare and severe presentation of polypharmacy overdose with a focus on massive bupropion and amitriptyline ingestion leading to seizures, cardiogenic shock, and loss of brainstem reflexes — ultimately exacerbated and prolonged due to a gastric pharmacobezoar, which resulted in delayed and continuous absorption of the ingested medications. Toxicology screens later confirmed elevated serum bupropion (600 ng/mL) and hydroxybupropion (3000 ng/mL) levels. Amitriptyline levels were not obtained.
Initial management followed standard toxicologic principles: airway protection, seizure control, hemodynamic support, and QRS narrowing with sodium bicarbonate. Continuous sedation with propofol was needed for seizure suppression, and a norepinephrine infusion was necessary for blood pressure stabilization. An echocardiogram revealed preserved cardiac systolic function. Due to the persistence of neurologic dysfunction and hemodynamic lability, the patient underwent upper endoscopy 18 hours post-ingestion.
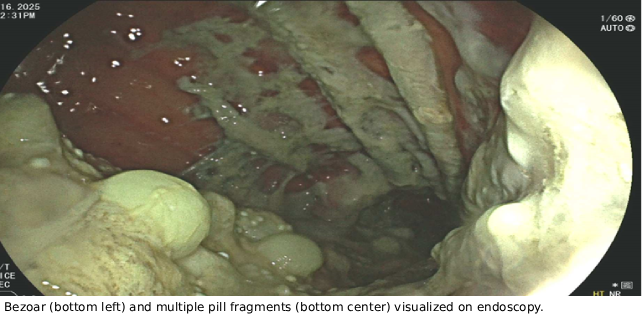
Upper endoscopy confirmed a bezoar composed of pill fragments and gastric contents. Whole bowel irrigation (WBI) with polyethylene glycol-electrolyte solution (PEG-ELS) at 2 L/hr and activated charcoal were initiated. This intervention led to a transient increase in QRS widening (174 ms) due to increased mobilization and absorption, which was treated with additional sodium bicarbonate to overcome the known cardiotoxic effects of both amitriptyline and bupropion. The absence of serum concentrations at this time limited confirmation but strongly supported ongoing absorption of both medications.
Discussion
Bupropion and amitriptyline both exert significant toxicologic effects in overdose due to their impact on neurotransmitter systems and cardiac conduction. Bupropion inhibits the reuptake of dopamine and norepinephrine, resulting in excessive catecholaminergic stimulation. Both agents block cardiac fast sodium channels and potassium channels, which can cause QRS and QTc prolongation. Additionally, tricyclic antidepressants like amitriptyline inhibit gap junctions between cardiomyocytes, disrupting electrical conduction, and potentially leading to arrhythmias or systolic dysfunction. These mechanisms collectively offer explanations for the observed seizures, cardiac conduction abnormalities, and central nervous system (CNS) depression in this patient.
Pages: 1 2 3 | Single Page




No Responses to “Case Report: Massive Amitriptyline and Bupropion Ingestion”