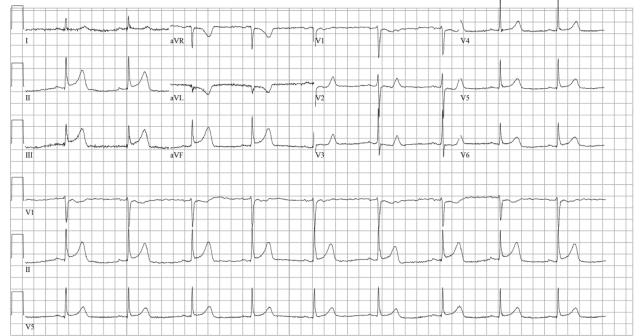
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During initial assessment, an ECG was obtained and revealed ST-segment elevation (STE) in the inferior leads with ST depression anteriorly.
Explore This Issue
ACEP Now: Vol 43 – No 12 – December 2024
FIGURE 1. Click to enlarge.
During assessment, the patient reported that a left heart catheterization six months prior indicated “spasms” but no coronary artery disease. Before nitroglycerin (NTG) could be administered, the patient became unresponsive and was transferred to the resuscitation bay, where the monitor revealed a ventricular fibrillation arrest. Advanced cardiac life support protocol was initiated, and the patient was intubated. During this time, a comprehensive chart review was conducted that revealed the patient had experienced two prior ventricular fibrillation arrests, both resolved with intracoronary NTG during left heart catheterization, showing severe dominant circumflex spasm resulting in 99 percent occlusion, which abated with intracoronary NTG.

FIGURE 2. Click to enlarge.
The patient was deemed to be in refractory fibrillation.
What Would You Do Next?
Attention was turned to the consideration of severe coronary vasospasm as the inciting event for cardiopulmonary arrest and the nidus for refractory ventricular fibrillation. The decision was made to communicate directly with the on-call interventional cardiologist with specific and direct intent to discuss the administration of intravenous (IV) NTG.

FIGURE 3A. Click to enlarge.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. Several minutes later, the patient again lost pulses, this time with pulseless electrical activity. After resuming CPR and administering an additional 400 mcg IV NTG, the patient achieved return of spontaneous circulation with sinus tachycardia. A repeat ECG was simultaneously performed that showed complete resolution of prior inferior elevation and anterior depression.
The patient was admitted to the cardiovascular intensive care unit and extubated the same day, neurologically intact. An urgent left heart catheterization revealed diffuse mild coronary atherosclerosis with normal ejection fraction. He was transferred out of the intensive care unit the next day and discharged shortly after, neurologically intact and at baseline.

FIGURE 3B. Click to enlarge.
Discussion
Since Prinzmetal and colleagues first described patients with coronary vasospasm as “variant angina” in 1959, the close relationship between this disorder and cardiac arrest has often been noted.1 Relatively little literature on the clinical characteristics and outcomes of out-of-hospital cardiac arrest (OHCA) patients complicated by coronary vasospasm exists beyond anecdotal reports, however. Overall, cardiac arrest in the setting of coronary vasospasm is thought to be relatively uncommon.2 OHCA patients with coronary vasospasm are typically younger, predominantly male, and often present with ventricular fibrillation or ventricular tachycardia as the initial rhythm. Traditional Advanced Cardiovascular Life Support (ACLS) medications, namely epinephrine, have been known to exacerbate coronary vasospasm.3 NTG is a potent coronary arterial dilator and is routinely used for ischemic discomfort in the setting of acute coronary syndrome, but is not typically deployed in the management of cardiac arrest. This case report documents the first known instance of using NTG during an emergency department resuscitation to treat a patient in cardiac arrest due to severe coronary artery vasospasm.
Pages: 1 2 3 | Single Page




No Responses to “Case Report: Coronary Vasospasm-Induced Cardiac Arrest”