
The Case
A 35-year-old white woman presented to the emergency department with a chief complaint of chest pain. She stated the chest pain began acutely, about 15 minutes prior to her arrival. The pain was sharp; radiated to her left arm; and was not accompanied by nausea, vomiting, fever, or chills. She had not missed any of her daily medications and had never experienced this type of discomfort before. She had no history of pulmonary embolism or deep vein thrombosis.
Explore This Issue
ACEP Now: Vol 40 – No 05 – May 2021The patient’s past medical history was significant for transposition of the great vessels, which required surgical repair at 4 months of age (a Senning procedure). She was known to have severe right ventricular (RV) dysfunction and was awaiting transplant workup. She also had a history of diabetes mellitus, hypothyroidism, atrial fibrillation, atrioventricular nodal re-entrant tachycardia (requiring previous ablation), and cardiac arrest with subsequent placement of an automated implantable cardioverter defibrillator. Her medications included rivaroxaban, insulin glargine, dulaglutide, levothyroxine, lisinopril, spironolactone, and metoprolol.
On exam, she was an obese woman who appeared slightly uncomfortable but in no acute distress. Vital signs were unremarkable: blood pressure 98/61, heart rate 84, temperature 97.3ºF, respiratory rate 18, and oxygen saturation 95 percent on room air. She had normal speech and mental status and had no diaphoresis. Her lungs were clear. A cardiac examination was normal. There was no pitting edema.
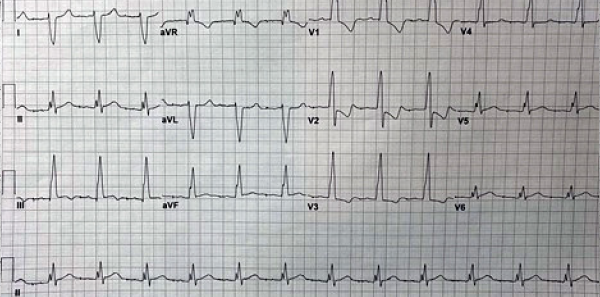
Figure 2: The patient’s initial ECG 10 minutes after presentation.
Her initial electrocardiogram (ECG) demonstrated an atrially paced rhythm with prolonged atrioventricular (AV) conduction and a bifascicular block, also evident on an ECG obtained one year prior to this incident (see Figures 1 and 2). Notably, the ST depression expected in the anterior leads with a right bundle branch block (RBBB) were changed, with less ST depression in V3 than before and no ST depression noted in V4. Though no pronounced ST elevations or depressions were noted, these findings were changes from the patient’s most recently known baseline and expected discordance in the ST segment in RBBB.
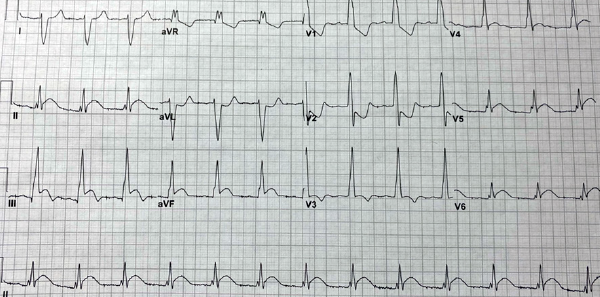
Figure 3: The patient’s ECG prior to cardiac catheterization, one hour after the initial ECG.
Alexandra Ferguson
Standard labs were obtained, with a complete blood count and basic metabolic panel within normal limits. A high-sensitivity initial troponin was normal.
At one hour, although her chest pain remained unchanged, her repeat troponin was elevated at 73 ng/L, up from 13 ng/L initially. A repeat ECG demonstrated ST segment elevations in leads II, III, AVF, and V6, with ST depression in V1 and V2 (see Figure 3). Given the concern for acute coronary syndrome (ACS), the patient was given a 324 mg dose of aspirin, intravenous heparin bolus, and infusion. She was seen by cardiology and was taken for emergent cardiac catheterization.
Cardiac catheterization demonstrated a complete embolic occlusion of the apical left anterior descending artery supplying the systemic right ventricle. Severe dilation of the right ventricle was also noted. The distal location of the embolus was not amenable to percutaneous coronary intervention.
The patient remained hemodynamically stable, and the decision was made to continue her on a heparin infusion and transfer her to the tertiary care facility for advanced cardiac care. There, she was evaluated for heart transplantation due to her worsening right ventricular dilation and systolic function.
Pages: 1 2 3 | Single Page




No Responses to “Case Report: Acute Coronary Syndrome Symptoms Require Repeat ECGs”