
A Structured Workup Matters
When a patient presents to the ED with an acute change in mental status, it’s our job as emergency physicians to uncover whether the etiology is treatable or life-threatening. A structured framework can help identify reversible causes and those who require escalation. The distinction between toxic-metabolic encephalopathy, focal neurologic deficit, and psychiatric dysfunction is more than just semantics — it’s a determinant of treatment and outcomes. Early clarity improves decision making, speeds treatment, and enhances safe disposition planning.
Explore This Issue
ACEP Now: January 2026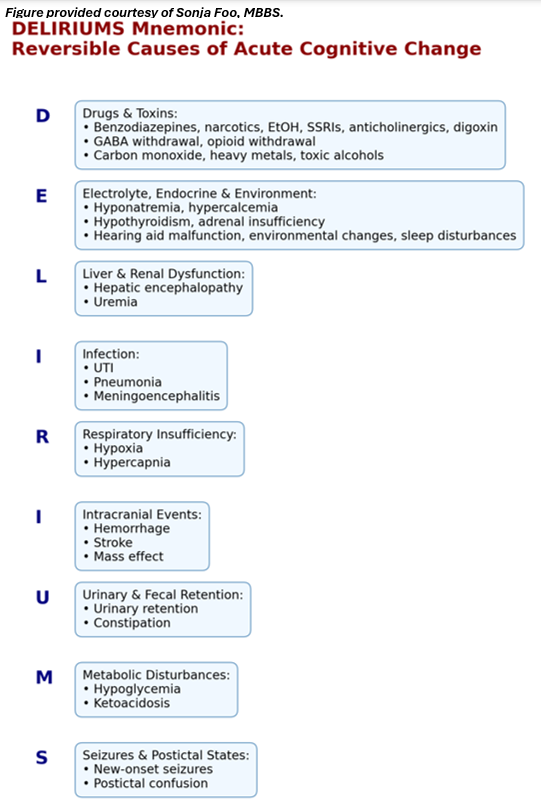
Click to enlarge.
Structured Workup: Reversible Causes
When delirium is identified — or even strongly suspected — it’s crucial to search for a cause. The DELIRIUM mnemonic offers a simple framework (see graphic).
Documentation: A Legal and Clinical Shield
Documenting that a patient is simply “confused” without further detail is not just medically inadequate; it could leave you legally exposed. Confusion is a symptom, not a diagnosis, and failing to clarify its nature, severity, and cause can expose physicians to significant liability, particularly when issues of competence and decision-making capacity arise.11-14 Courts have repeatedly identified gaps in documentation of altered mental status as evidence of substandard care, especially in cases involving unsafe discharges, failure to obtain informed consent, or missed diagnoses like sepsis, hypoxia, or toxic-metabolic encephalopathy.15
Instead of vague descriptors, clinicians should clearly articulate:
- Baseline versus current mental status (with collateral when possible)
- Objective findings (e.g., inattention, fluctuating alertness, or disorganized thinking)
- Clinical decision tools (e.g., 4AT score and interpretation) to anchor your exam in a validated framework
- Suspected etiology (e.g., infection, medications, or organ dysfunction)
- Disposition and treatment plan (e.g., acute interventions, consults, and decisions around admission versus outpatient follow-up)
A clear documentation of mental status changes reinforces clinical reasoning, supports safe care, protects legally, and ensures billing compliance. How you document influences how you deliver care and how that care is judged.
Future Directions
The ED is chaotic. We’re pressed for time, faced with frequent interruptions, and often lack baseline context (especially overnight). This is precisely why and where structure matters most. A brief screening checklist shouldn’t be a burden but instead a safeguard. Integrating 4AT into triage or nursing workflows, prompting collateral questions (if available), and adopting the DELIRIUMS mnemonic in electronic health records smart phrases are low-cost yet high‑impact strategies. Better structure results in better care with minimal workflow disruption.
Conclusion
We’re no strangers to the nuances of detecting delirium in the chaotic, fast-paced setting of the ED. Just the other day, a 78-year-old woman presented to my ED with a chief complaint of “confusion.” Upon evaluation, she was alert, oriented, and perfectly conversational. She insisted she felt fine and had only come because her daughter was worried. However, it was the collateral history that told the real story: the night before, she’d been disoriented, wandering her own home, convinced she was somewhere unfamiliar. Her workup revealed a urinary tract infection that I was able to quickly identify and treat.
Pages: 1 2 3 4 | Single Page



No Responses to “A Practical Guide to Diagnosing Delirium and Acute Cognitive Change in the ED”